|
STEM CELLS |
|
|
Laurance Johnston, Ph.D.
Sponsor: Institute of Spinal Cord Injury, Iceland |
| |
NORTH AMERICA (USA)
1) Geron (USA)
2) TCA Cellular
Therapy (USA)
3) Medistem (USA,
Panama, Costa Rica)
MEXICO, SOUTH AMERICA
1)
Dr. Tarcisio Barros
(Brazil)
2) Dr. Gustavo Moviglia
(Argentina)
3) Luis Geffner
(Ecuador)
4) Dr. Fernando Callera
(Brazil)
5)
Dr. Emilio Jacques
(Mexico)
6)
Medra
(Dominican Republic)
EUROPE
1)
Dr. Eva Sykova
(Czech Republic)
2)
Dr. Cornelis
Kleinbloesem (Netherlands, Germany)
3)
Dr. Venceslav Bussarsky
(Bulgaria)
4) Dr. Robert Trossel
(Netherlands)
5) Dr. Armin Curt
(Switzerland)
RUSSIA
1)
Dr. Andrey Bryukhovetskiy
(Russia)
2)
Dr. Samuil Rabinovich
(Russia)
3) Dr. E. R. Chernykh
(Russia)
ASIA - CHINA, KOREA & JAPAN
1)
Dr. K-S Kang (South
Korea)
2)
Dr. Yoon Ha (South Korea)
3)
Dr. Yongfu Zhang
(China)
4) Dr. Fukuki Saito
(Japan)
5) Beike Biotechnology
(China)
6) Tiantan Puhua
Hospital (China)
7) China Network
ASIA - INDIA & OTHER
1)
Dr.
Geeta Shroff (India)
2) Dr.
Satish Totey (India)
3) Dr. R. Ravi Kumar
(India)
4) Dr. Adeeb Al-Zoubi
(Jordon)
5) Dr. Haluk Deda (Turkey)
6) Dr. Himanshu Bansal
(India)
7)
Dr. Sunil Waghmare
(India)
8) Dr. Alok Sharma
(India)
9) Dr. Ayhan Attar
(Turkey)
AFRICA
1) Dr. Nirmeen Kishk
OTHER
1)
Advance Cell
Therapeutics

NORTH AMERICA (USA)
1) Geron
Corporation (USA)has initiated a preliminary study evaluating
the safety of transplanting hESC-derived cells in 8-10 individuals who
had sustained thoracic T3-T10 injuries within 7-14 days of enrollment.
Before transplantation, the hESCs will be induced
to differentiate into oligodendrocyte progenitor cells (OPCs), which, as
discussed in the stem-cell introduction, can evolve into
oligodendrocytes, a myelin–producing neuronal support cell. Basically,
myelin insulates the neuron, controlling signal-propagating ion flow in
and out of the cell. After injury, many neurons remain intact but have
lost their insulating myelin sheath and, hence, are dysfunctional. The
goal of Geron’s approach is to restore function by remyelinating and
turning on these neurons.
The cells will be injected into the cord’s area of
injury. To prevent potential immunological rejection of the transplanted
cells, the patients will take anti-rejection drugs for several months,
which some believe could be a potential risk in itself during this
sensitive recovery phase. Although the study’s primary endpoint is
safety, functional improvements in the trunk or lower extremities will
also be assessed.
For awhile, the US Food and Drug Administration
(FDA) blocked the study from proceeding because rat studies suggested
that the transplanted cells form microcysts in the spinal cord. After
FDA lifted this regulatory block, recruitment started in the fall of
2010.
In June 2011, Geron staff presented preliminary
data on the first two patients to be recruited, both who possessed
neurologically complete thoracic injuries. Two million cells were
injected into the injury site between 7 and 14 days after injury. As
indicated before, to prevent potential rejection of the transplanted
cells, an immune-suppression drug was administered for 60 days. At the
time of the report, one patient had been followed for 180 days and the
other for seven days. Overall, no surgical complications were noted,
and, in the longer-observed patient, there was no evidence of immune
rejection of the transplanted cells 30 days after
immune-suppression-drug administration had been stopped.
The proposed trial is built upon a foundation of
animal research carried out by Dr. Hans Keirstead and colleagues
(USA), who have transplanted hESC-derived OPCs into rats with a
contusion injury, the sort of injury most commonly observed in humans.
 To
compare the effectiveness of such transplantation in acute and chronic
injury, 1.5-million OPCs were injected into rats seven days and 10
months after injury (i.e., acute and chronic injury phase,
respectively). All animals received an anti-rejection drug (cyclosporine
A) starting a day before transplantation and proceeding to the end of
the study. To
compare the effectiveness of such transplantation in acute and chronic
injury, 1.5-million OPCs were injected into rats seven days and 10
months after injury (i.e., acute and chronic injury phase,
respectively). All animals received an anti-rejection drug (cyclosporine
A) starting a day before transplantation and proceeding to the end of
the study.
In both the seven-day and 10-month rats, the
transplanted cells survived, differentiated into oligodendrocytes, and
migrated short distances in the cord. However, the seven-day, acutely
injured rats showed significant remyelination and improved locomotor
ability, while the 10-month, chronically injured rats had no such
improvement. Apparently, the formation of injury-site scar tissue over
time inhibits the remyelination potential of the transplanted cells.
These results are the reason why Geron’s trial will include only
individuals with acute and not chronic injury.
2)
In 2010, TCA
Cellular Therapy
(USA) announced the initiation of a
phase-1 study evaluating the safety and tolerability of an intrathecal
infusion (i.e., lumbar puncture) of bone-marrow-derived, mesenchymal
stem cells. The cells will be isolated from the patient’s bone marrow
(i.e., autologous), purified, and amplified in culture before being
transplanted back into the patient. Recruited subjects must have ASIA-A
complete injuries below the cervical C5 level and been injured between
two weeks and 60 months before recruitment.
3)
In 2010, investigators associated with
Medistem, Inc
(USA, Panama, Costa Rica) reported the results of treating a 29-year-old
male with an ASIA-A complete injury (see appendix) at the T12-L1 level
with several umbilical-cord-associated stem cells. Cells were
transplanted into the intrathecal space surrounding the spinal cord in
three cycles 5, 8, and 14 months after injury. During the last cycle,
the cells were also injected intravenously. At the time of his final
assessment a half year after the last treatment cycle, the patient had
improved to an ASIA-D incomplete-injury classification (see appendix),
had recovered some bowel, bladder, and sexual function, and had less
neuropathic pain. No adverse effects were observed.
SOUTH AMERICA, MEXICO
1) Dr.
Tarcisio Barros et al (Sao Paulo, Brazil) have infused
bone-marrow-derived stem cells into the spinal artery closest to the
injury site in 32 subjects with clinically complete injuries (2-12 years
post injury). The stems cells were isolated from the patient’s own blood
after treatment with a drug that stimulates the bone-marrow production of
these cells and, in turn, their spillover into the blood. After one-year follow-up, 18 patients have shown
improvement in electrophysiological neuronal conduction, which, in some
cases, has been translated into functional improvement. (Photo:
Drs. Erika & Tarcisio Barros).
spillover into the blood. After one-year follow-up, 18 patients have shown
improvement in electrophysiological neuronal conduction, which, in some
cases, has been translated into functional improvement. (Photo:
Drs. Erika & Tarcisio Barros).
The results of the completed study were reported in
a 2009 article. Cumulatively, these University of San Paulo
investigators had infused such stem cells into the spinal-cord-serving
arteries of 39 patients between 2002 and 2004. Of these patients, 11
were women, and 28 were men. Six had injuries between the cervical C2-C4
vertebral level, eight between the C5 and thoracic T1 level, and 25
between the T2 and lumbar L1 level. Injuries were caused by motor
vehicle accidents (24), sports (7), and motorcycle/aircraft accidents
(2). All patients were at least two years post injury. In other words,
they all had chronic injuries, in which little additional recovery is
routinely expected and, as a result, any improvements accruing are most
likely due to the intervention.
After treatment, the patients were followed at
six-month intervals for 2.5 years using electrophysiological
measurements of nerve conduction. With these measurements, the lower limbs would be
stimulated and any ensuing response measured in the brain. Although no
patient could generate such a response before stem-cell treatment, 26
were able to do so afterwards. On average, this renewed nerve-conduction
started nine to ten months after treatment.
2) Dr.
Gustavo Moviglia et al (Argentina) has treated two individuals with bone-marrow-derived mesenchymal stem cells that have been transformed into neural stem cells
by culturing with patient-derived autoimmune cells (Cytotherapy 8
2006).
 Compared to other programs, the science behind this program has an
additional, more-difficult-to-understand dimension. Specifically, it
combines a stem-cell approach with some of the immunological principles
that underlie Dr. Michal Schwartz’ “activated macrophage” program for
acute SCI discussed later. Compared to other programs, the science behind this program has an
additional, more-difficult-to-understand dimension. Specifically, it
combines a stem-cell approach with some of the immunological principles
that underlie Dr. Michal Schwartz’ “activated macrophage” program for
acute SCI discussed later.
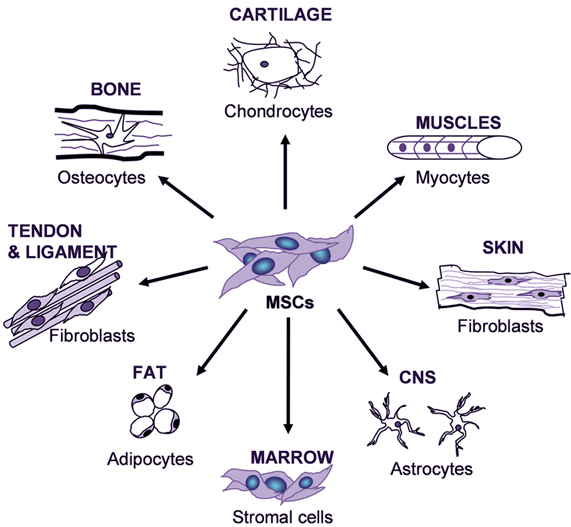
In this program, mesenchymal stem cells were obtained
from the marrow of the patient’s iliac crest (i.e., hip) bone, a location
where a large quantity of marrow is concentrated. Called the
jack-of-all-trades stem cell, mesenchymal stem cells have the potential to
differentiate into a wide variety of cell types. After further
purification, these stem cells were transformed into neural stem
cells by culturing them with autoimmune cells previously isolated from the
patient. Because all cells are from the patient (i.e., autologous), there
is little rejection potential when implanted back into the patient.
Before stem-cell implantation, the previously
isolated autoimmune cells were intravenously infused into the patient.
This infusion primes the injury site by generating an inflammation
response, creating a more receptive microenvironment for the introduced
stem cells. Two days later, the processed mesenchymal/neural stem cells
were infused into an artery serving the injury-site area.
The first patient treated was a 19-year-old male who
had sustained a thoracic T-8 injury eight months before treatment from a
car accident. He received two stem-cell infusions separated by three
months. Electrophysiological measurements suggested improved nerve
conduction through the injury site, and MRI (magnetic resonance imaging)
evaluations indicated increased spinal-cord diameter. After the second
treatment, his coordination and walking ability improved. Reportedly, he
regained function to the sacral S-1 level.
The second patient was a 21-year-old woman with a
cervical C3-5 injury cause by a car accident 30 months before
implantation. After one treatment, both electrophysiological and MRI
assessments suggested improvements, and the patient regained upper body
strength and control, including hand function. Reportedly, she regained
function to the thoracic T1-2 level.
Building upon this research, in 2009, Moviglia and
associates reported the results of treating eight patients with chronic,
complete injuries with three different cell therapies. Although
details were sketchy, the process seemed to be similar to that discussed
above except an additional preparatory cell therapy was added.
First, to enhance the all-important growth and
development of new blood vessels (called angiogenesis) to the injury
site, angiogenesis-promoting bone-marrow-derived stem cells were infused
through an artery servicing the area. Second, 18-days later,
spinal-cord-specific immune cells were introduced into the patients, the
purpose of which was to open the blood-brain barrier and generate a
microenvironment more suitable for the implantation of reparative stem
cells. Third, autologous (i.e., isolated from the patient) neural stem
cells were infused into an artery servicing the injury area. These cell
transplantations were followed by neuro-rehabilitation programs designed
to maximize functional recovery.
After treatment, five patients progressed from
complete ASIA-A to incomplete ASIA-D injuries (see glossary) and
regained, to varying degrees, standing and walking ability. Two others
patients showed some motor and sensory improvements. One patient was not
evaluated. No serious side effects were observed.
3)
Reported at the 13th Annual Meeting of the
International Society for Cellular Therapy (June 2007),
Dr. Luis Geffner (Ecuador) and colleagues have
treated 25 patients with stem cells isolated from the patients’ own bone
marrow (i.e., autologous). The time elapsing from injury to treatment
ranged from 0.5 months to 22 years (average 4 years). Because
considerable functional improvement may accrue without any intervention
in the first year post-injury, any improvement of subjects treated soon
after injury confounds overall results. Approximately, 1.2-million stem
cells per kilogram body weight were implanted, and four to seven days later, a
long-term rehabilitation program was started. Improvement was assessed
by a variety of means, including electrophysiological evaluations of
nerve conduction, MRI imaging of the spinal cord, urinary function,
spasticity, walking ability, and ASIA impairment scales. According to
the investigators: “Patients demonstrated improvements in sensitivity,
motility, bladder sensation, even controlling sphincters, erection, and
ejaculation. Fifteen patients (60%) could stand up, 10 (40%) could walk
on the parallels with braces, 7 (28%) could walk without braces, and 4
(16%) could walk with crutches.” Although it is unclear how this data
compares to pretreatment function, the ASIA scores improved considerably
after the intervention. No adverse effects were observed, and no
patient deteriorated due to treatment.
In 2008, Geffner et al reported that they had
cumulatively treated 52 patients with SCI with autologous bone-marrow
stem cells isolated from the patient’s iliac bone (largest bone of the
pelvis). The investigators specifically discussed eight cases (7 men),
who had been followed for the longest time periods. Four individuals had
more acute injuries sustained 5 days, 13 days, 1.5 months, and 7 months
before treatment; and four had chronic injuries sustained 6, 6, 7, and
22-years prior to treatment. Injuries ranged from the thoracic T4 to
T12 level and were caused by gunshots (4), falls (3), and a car accident
(1).
Before transplantation, a laminectomy was performed
to expose the spinal cord, the scar tissue was carefully removed, and
the cord detethered. Cumulatively, 90-million cells were implanted into
each patient. To increase the likelihood that they would reach their
target, the cells were introduced into each patient by three different
routes. Specifically, 1) 20 milliliters of cell suspension were injected
in numerous locations in and around the injury site; 2) after suturing
shut the dura membrane surrounding the exposed cord, another 30
milliliters was infused into the spinal canal; and 3) a final 30
milliliters administered intravenously.
Patients were evaluated before treatment and
6-months, 1-year, and 2-years afterwards using a variety of assessments,
including the commonly used ASIA or Frankel impairment scales,
spasticity assessments, quality-of-life evaluations, bladder function,
and MRI imaging. To varying degrees, all patients recovered some
function, even the four with long-term injuries in which additional
functional recovery is considered unusual.
The researchers emphasize the potential importance
of the angiogenesis-promoting properties of these stem cells. They
hypothesize that improved blood flow and oxygen supply within the injury
area may have contributed to the functional improvements seen in these
patients.
4) Dr.
Fernando Callera’s team (Brazil) assessed the safety of
transplanting patient-derived, bone-marrow stem cells into 10 patients
via lumbar puncture. Seven had paraplegia and three had quadriplegia;
mean age was 24; and the time lapsing since injury averaged three years.
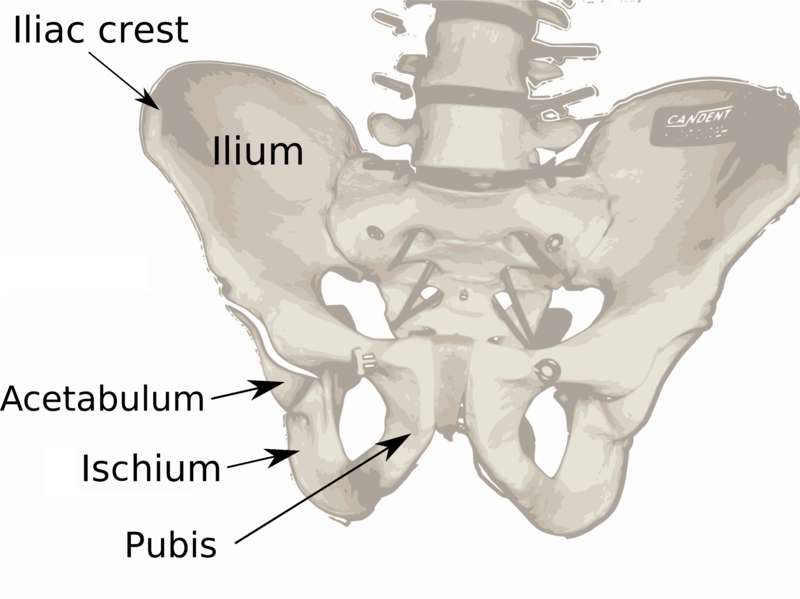
To stimulate stem-cell production by the bone marrow, patients were
given granulocyte macrophage-colony stimulating factor (GMCSF) for five
days. On day six, 100 milliliters of bone-marrow tissue were aspirated
from the pelvic bone’s iliac crest (see illustration above), and the
stem cells isolated. Four hours after aspiration, ~100-million cells
were transplanted via lumbar puncture. After following the patients for
12 weeks, the investigators concluded the “procedure was feasible, safe,
and well tolerated.”
5) Dr.
Emilio Jacques (Mexico) has transplanted umbilical
cord stem cells into the injury area. Based on limited information,
Jacques’ procedures apparently removed the scar tissue by laser,
decompressed the spinal cord, injected stem cells into the injury area,
and placed patient-derived fatty tissue over the injury area to minimize
scar-tissue formation. The procedure is followed by monthly stem-cell
injections into surrounding muscles. Sources indicate that Jacques has
also started transplanting embryonic stem cells.
One patient who sustained a T5-9 injury about a year
and half before treatment briefly described to this report author some of
the functional improvement that accrued three months after surgery.
Specifically, he feels touch two inches below the T9 level and pressure
all the way down to his waist. Furthermore, he can peddle a bike on his
own for over 30 minutes, move his hips, push 25 pounds with his legs, and
using a harness and treadmill, swing his legs forward.
Jacques’ stem-cell procedures were summarized in a
2005 talk at the 2005 International Congress of Surgeons in Acapulco,
Mexico. The submitted abstract indicated that he implanted the undefined
stem cells “exactly in the spinal cord injured zone, combined with
post-operative use of neuro-muscular rehabilitation, electro-acupuncture,
infrared laser, and 4AP.” (A conduction-enhancing drug)
Of the 59 treated patients (average age 21), 51% and
49% were male and female, respectively; 50 and 9 had incomplete and
complete injuries, respectively; and 52%, 38%, and 10% sustained cervical,
thoracic, and lumbar/sacral injuries, respectively. Jacques reported that
68% “gained sensory and motor levels; 16% gained only motor level and the
remaining 16% were still the same.” Patients who had sustained lower level
injuries, who were younger, and who had less time elapsing since injury
did the best.
6) Medra, Inc./Stem
Cell of America
under Dr. William Rader’s medical direction, provides a fetal
stem-cell program for a wide range of neurological and other disorders,
including SCI. Although headquartered in Malibu,
California, the surgeries are carried out in the Dominican Republic and
Mexico. Very
few specifics relevant to SCI-related procedures are available.
Derived from elective abortions, fetal hematopoietic stem cells are
apparently administered intravenously and fetal neuronal stem cells
subcutaneously into the lymph nodes. The program claims that these cells
will migrate to the location where they are needed and also release
function-restoring growth factors. The program states that the key
advantage of using fetal stem cells over, for example, bone-marrow stem
cells is that the undifferentiated nature of the former minimizes
immunological rejection. This claim, however, ignores the fact that a
number of emerging SCI-related stem-cell programs (see above) use
autologous stem cells (i.e., isolated from the patient) which are even
more immunologically compatible than fetal cells.
When contacted several times by the author
of this report, the company did not respond.
EUROPE
1) Dr. Eva
Sykova and colleagues (Prague,
Czech Republic) have implanted autologous, bone-marrow stem cells
harvested from the iliac bone (i.e., pelvis) into 20 patients.
 Eight were subacute, receiving treatment
within 10-33 days of injury; and 12 were defined as chronic, receiving
treatment 2-18 months after injury. Soon after harvesting, about
150-million cells cells were
reintroduced into the patient through the vertebral artery or
intravenously. With the subacute patients, four were treated by each
route; with the chronic patients, two and 10 received cells via the artery
and intravenous route, respectively. Eight were subacute, receiving treatment
within 10-33 days of injury; and 12 were defined as chronic, receiving
treatment 2-18 months after injury. Soon after harvesting, about
150-million cells cells were
reintroduced into the patient through the vertebral artery or
intravenously. With the subacute patients, four were treated by each
route; with the chronic patients, two and 10 received cells via the artery
and intravenous route, respectively.
Patients were assessed periodically
by various electrophysiological measurements and ASIA-impairment scales.
Improvements were noted in 1) all subacute patients receiving the cells
via the vertebral artery but only one receiving the cells intravenously,
and 2) one of the two chronic patients receiving the cells via the
vertebral artery. Of the patients who improved their ASIA grades, most
advanced from grade A to B, and one from grade B to D (i.e., scale ranging
from A, most paralyzed, to E, complete recovery). Although Sykova is
cautious in over-interpreting these preliminary results, she believes more
benefits accrued when the treatment was done sooner after injury and using
the vertebral artery route, which introduces cells closer to the injury
site.
In a 2009 update,
the number of patients treated by these procedures had grown to 36.
2) Dr.
Cornelis Kleinbloesem created a stem-cell oriented company
Cells4Health with headquarters in Netherlands but using Turkish surgeons
and facilities. The C4H program
collected bone-marrow cells from the patient through a puncture in the
iliac crest bone (pelvis) in which a large quantity of bone marrow
is concentrated. The isolated stem and other bone-marrow cells were
processed through a proprietary process.
The cells were then injected into the
patient’s spinal cord at the lesion area through 20-40 microinjections.
Cumulatively, about two-milliliters of the stem-cell preparation,
corresponding to about 10-20 million cells, were injected above, below,
and around the injury site using an insulin needle. In some later
cases, cells were also intrathecally (into the spinal canal) or
intravenously injected.
At least 18 patients
with SCI had been treated under this C4H program. Of the first nine
patients with chronic SCI treated, eight reportedly had positive
results. In three of the first four treated in February, 2005, MRI
imaging indicated that the lesion size was reduced by half three months
after surgery, data suggesting the creation of new neural cells and
supporting structure.
Reportedly, cell transplantation restored
some function and sensation in three of these four initial patients.
Two to three months after transplantation, the first patient, who
sustained a T6-complete injury four years earlier from a car accident,
reportedly recovered function to the T12- L1 level and was able to move
legs, walk a few steps using a walker, and stand. The second patient,
who had sustained a complete cervical-level C5-6 injury seven
months earlier, a month and half after surgery was said to be able to
move legs and fingers and feel toes, and regained rectal and bladder
sensation. Several months after transplantation, the third patient, who
sustained a complete C5-6 injury nine months earlier from a surgical
complication, reportedly regained his ability to stand, ambulate using a
walker with leg braces, and write. Also, his sensation returned to near
normal, and he regained rectal control. The fourth patient accrued no
benefit, perhaps because his spinal cord turned out to be transected not
compressed.
Many of the
results were reported by C4H.
Independent sources have portrayed a less promising picture with many
patients not gaining and some even losing function.
More recently, Kleinbloesem and colleagues have
created the XCell-Center located in Germany, which appears to carry out
many similar procedures for a variety of disorders including SCI.
Specifically, stem-cell-rich bone marrow is obtained from the patient’s
hip bone, the stem cells are processed from this marrow, and
transplanted back into the patient’s injured cord after exposure by a
surgical laminectomy or through a less invasive lumbar puncture into the
spinal fluid. The program claims a 60% success rate in restoring some
function.
According to Xcell-Center follow-up data of 162
patients with SCI (March 2010), ~57% reported improvements after stem
cells were transplanted by lumbar puncture. Of these patients, ~38%, 36
%, and 30% reported improved bladder, bowel, and sexual function,
respectively; and 53% and 51% reported decreased neurogenic pain and
muscle spasticity, respectively. In the 46 patients who completed pre-
and post-treatment ASIA motor and sensory examinations, the average
motor score increased by six points and the average sensory score by 11
points.
In April 2011,
Xcell Center ceased operations in response to changes in German
regulatory policy on stem cells. Kleinbloesem has now relocated
operations to Lebanon.
3) Dr.
Venceslav Bussarsky et al (Bulgaria) have treated 115 patients
with chronic SCI with autologous stem cells and growth factors isolated
from the patient’s bone marrow. Patient age ranged from 18 to 65
(average 43) years. Approximately, 40-million cells were intrathecally
infused into the space surrounding the spinal cord, a procedure repeated
nine months later. Various MRI, neurological, and psychological tests
were done before and three months after each treatment. Although the
study lacked a control group for comparison, improvements in sensory and
motor function was noted in 105 patients.
4)Dr. Robert
Trossel (Netherlands) has treated individuals with SCI with umbilical stem cells. Although
specifics are
scanty, one press report briefly described Trossel’s treatment of a woman with a high-level injury. In this case,
1.5-million stem cells were intravenously injected at the base of her
skull where she was injured and at five other locations down each side of
her neck. Trossel’s therapy has generated
controversy.
5) Dr. Armin
Curt (Switzerland) has initiated a phase I/II clinical tr ial
transplanting human central nervous system stem cells into individuals
with complete and incomplete thoracic injuries who became injured three
to twelve months earlier. Although taking place in Switzerland, the
trial it is being sponsored and the stem cells provided by StemCells,
Inc headquartered in California, USA. The trial will use stem cells
derived from aborted fetuses. Unlike embryonic stem cells, these cells
have already differentiated into central nervous system cells.
Preliminary results reported at
the 2012 meeting of the International Spinal Cord Society indicated that
two of the first three study subjects had regained some sensation below
the level of their injuries. ial
transplanting human central nervous system stem cells into individuals
with complete and incomplete thoracic injuries who became injured three
to twelve months earlier. Although taking place in Switzerland, the
trial it is being sponsored and the stem cells provided by StemCells,
Inc headquartered in California, USA. The trial will use stem cells
derived from aborted fetuses. Unlike embryonic stem cells, these cells
have already differentiated into central nervous system cells.
Preliminary results reported at
the 2012 meeting of the International Spinal Cord Society indicated that
two of the first three study subjects had regained some sensation below
the level of their injuries.
RUSSIA
1) Dr. Andrey
Bryukhovetskiy (Moscow, Russia), former director of the Russian
Navy’s Neurology Department, has transpla nted
both embryonic/fetal stem cells and autologous (i.e., from the
patient) adult stem cells into patients with chronic SCI. In addition in
some patients, Bryukhovetskiy has transplanted autologous olfactory
ensheathing cells (OECs) using procedures developed by England’s Dr.
Geoffrey Raisman. Although not technically stem cells, as discussed above,
OECs have considerable regeneration potential and have been the focus of
much attention in the SCI research community. nted
both embryonic/fetal stem cells and autologous (i.e., from the
patient) adult stem cells into patients with chronic SCI. In addition in
some patients, Bryukhovetskiy has transplanted autologous olfactory
ensheathing cells (OECs) using procedures developed by England’s Dr.
Geoffrey Raisman. Although not technically stem cells, as discussed above,
OECs have considerable regeneration potential and have been the focus of
much attention in the SCI research community.
Bryukhovetsiy no longer uses embryonic/fetal
stem cells due to the ethical controversy surrounding their use, their
rejection potential, and, most importantly, his belief that autologous,
adult stem cells are more effective.
Basically, Bryukhovetskiy's transplantation
procedures can be categorized as follows:
Embryonic Cells: In 1996, the Russian Health
Ministry authorized Bryukhovetskiy to carry out limited clinical trials in
SCI. In these early trials, stem cells, neurons, and glia obtained from a
various tissues, including 12-week-old human fetuses, were transplanted
into the spinal cord/fluid of 17 patients with SCI. Their ages ranged from
16-52 (average 30) years, and the time interval between injury and
transplantation ranged from 1-20 (average 5) years. Six, ten, and one had
cervical, thoracic, and lumbar injuries respectively. In addition to cell
transplantation, all had a variety of other procedures performed depending
upon their unique injuries.
Before treatment, 14 subjects were ASIA grade A and
three were grade B. After transplantation (0.5 - 3-year follow-up period),
four were grade A, five grade B, and seven grade C. Fifteen had some
sensory improvement, seven had motor improvement, and 12 had improved
bladder function.
SpheroGel & Autologous Cells: Bryukhovetskiy’s
team has implanted SpheroGel (a biodegradable polymer matrix) with
embedded cells in six patients who required reconstructive surgeries. In
three, hematopoietic stem cells were embedded, and, in the three others,
olfactory cells. At follow-up (3-8 months), two grade-A patients had
improved to grade C, and one had advanced to grade B. In one patient
(grade B initially), there was no improvement.
Intrathecal Stem-Cell Transfusion: The
intrathecal transfusion of autologous hematopoietic stem cells is the
procedure most currently used. Basically, in this relatively
straight-forward procedure involving no surgery, the patient’s stem cells
are collected without anesthesia and stored with viability until they are
transfused back into the patient.
To stimulate hematopoietic stem-cell production and,
in turn, cell accumulation in the blood, patients typically received eight
subcutaneous injections over four days of granulocytic colony-stimulating
factor, a drug also called Neupogen® or Filgrastim. On day
five, the patient is hooked up to a blood separator. Over 3-4 hours, blood
is drawn from a vein, processed by the separator, which isolates the stems
cells, and returned through another vein.
The collected stem cells are concentrated by
centrifugation and slowly frozen in liquid nitrogen (-170o
centigrade) in the presence of dimethyl sulfoxide (DMSO), a
cryopreservative that allows cells to be frozen with minimal damage. Care
is taken to check for infections so that they will not be later introduced
behind the protective blood-brain barrier during transfusion.
At the time of transfusion, the stem-cell suspension
is thawed and about 5.3-million cells injected intrathecally into the
subarachnoid space (i.e., into the spinal fluid) through a L3-L4 lumbar
puncture using a local anesthetic (photo). The procedure, which I
observed, is quick and straightforward. The patient can repeat the
transfusion in two months. Bryukhovetskiy believes multiple transfusions
enhance functional recovery.
In contrast to hematopoietic stem cells, positive
results have been limited with the intrathecal transfusion of olfactory
cells, previously isolated and cultured from the patient’s nasal tissue.
Although Bryukhovetskiy’s team has collected stem
cells from about 120 patients, for a variety of reasons, including the
presence of latent infections, only about 60 have had cells reintroduced.
Of these 60, 18 have had the recommended multiple transfusions. In turn,
61% of the 18 showed some functional recovery, in some cases dramatic.
Because most patients’ transfusions were relatively
recent at the time of this report, it is too early to assess long-term
benefit. Early improvements are unlikely caused by comparatively slow
neuronal regeneration or remyelination processes and are probably
triggered by altering the injury site’s environment through the secretion
of growth factors and other molecules.
Bryukhovetskiy hypothesizes that the stem-cells’
regenerative effects are mediated through an important growth factor
called ciliary neurotrophic factor (CNTF) and its interaction with
a key transmembrane receptor called gp130. This interaction, in
turn, influences cell differentiation.
In 2012, Dr. Bryukhovetskiy reported the
electrophysiological outcomes of treating 20 individuals with injuries
at the cervical C4-8 level with autologous (i.e., from the patient)
hematopoietic stem cells. These hematopoietic stem cells have the
potential to differentiate into myelin-producing cells which, in turn,
have the capability to replace the insulating myelin that is often lost
in injury-damaged neurons.
Of the 20 patients, 15 were men and 5 were women;
age ranged from 18 to 55 (average 32) years; and the time lapsing since
injury varied from 1 to 9 (average 3) years. Patient stem cells were
obtained as described above. Specifically, after several days of dosing
with a stem-cell-stimulating drug, stem cells were isolated from the
patient’s blood and frozen until it was ready to transfuse them back
into the patient. The cells were injected intrathecally into the spinal
fluid (i.e., lumbar puncture) twice over an 8-day period. After 3-5
months, the next two stem-cell doses were given, and the cycle repeated.
The duration of treatment varied from 1.5 to 2.5 years.
Periodically, electrophysiological measurements
were performed on the patients, including somatosensory and motor evoked
potentials (defined in appendix). Basically, these measurements assessed
the amount of signal getting through the injured spinal cord. More
conduction after stem-cell therapy would suggest some restoration of
neuronal function. Indeed, the results indicated that many of the
patients accrued some improvement in conduction after treatment.
2) Dr.
Samuil Rabinovich and colleagues (Novosibirsk, Russia) have
transplanted various combinations of fetal OECs, cells from nervous and
hematopoietic tissues, and spinal cord fragments into the injury site of
15 patients (Biomed Pharmacother 57(9), 2003). Ranging in age from
18 to 52, patients were one-month to six-years post injury and had
complete, Frankel grade-A injuries (Frankel classification evolved into
today’s ASIA scale). Each patient received one to four cell
transplantations at various times, and was followed at least 1.5 years.
Improvements were noted in 11 of 15 patients. Six improved to grade-C,
incomplete level, and five were able to walk with crutches. In general,
patients who had the transplantations sooner after injury accrued the most
benefit.
According to an updating report posted on the
investigators’ website www.transplantation.ru,
122 patients have been treated with a procedure in which the injury site
is filled with a gel containing fetal stem cells. The initial
transplantation is followed later by one or more additional
transplantations of the cells underneath the spinal-cord membrane (i.e.,
subarachnoid). The time between injury and surgical transplantation
ranged from several months to five years.
The outcomes for these patients are reported in the
table below. As can be seen, many patients regained some function,
although some were treated in a period after injury in which additional
functional recovery is not uncommon.
|
Neurological status in terms of ASIA definition
before transplantation |
Neurological status after transplantation |
|
A |
B |
C |
D |
|
A
(73 patients) |
31% |
48% |
18% |
3% |
|
B
(49 patients) |
- |
78% |
22% |
- |
In 2010, Dr. Rabinovich and colleagues reported the
long-term recovery results of fetal cell transplantation in 43 patients
with SCI. Of these patients, 11 were men and 32 were women; and 22, 12,
and 9 had cervical, upper thoracic, and lower thoracic/lumbar injuries,
respectively. Three patients were less than 20 years old, 23 were 20-29
years old, 13 were 30-39 years old, and 4 were older than 40. The time
from injury to transplantation was two to five years in 37 patients
(also 3 < 1 year; 3 > 5 years).
The transplanted fetal cells were isolated from the
brain and liver of 16-22-week aborted fetuses and were composed of both
fetal nervous and hematopoietic (see glossary) cells. These cells were
repeatedly transplanted into the patient’s cerebrospinal fluid by lumbar
puncture. In spite of the concerns surrounding the use of fetal cells
for transplantation, these investigators actually believe that their use
has advantages over autologous cells (i.e., isolated from the patient)
because these fetal cells contain “the whole spectrum of brain cells at
different stages of differentiation…with high growth potential capable
of integrating into the neuronal networks of recipient."
Improvements were primarily measured using the FIM
scale (Functional Independence Measure), which evaluates everyday
functional independence. Using this assessment, 49% of patients who
were followed for at least three years reported improvements. Greater
benefits were observed in patients receiving cell transplantation within
the first two years after injury and in younger recipients.
3) Dr.
Helena Chernykh
and colleagues (Russia) transplanted autologous bone-marrow stem cells
into the spinal cord of 18 patients with SCI undergoing a surgery to
treat cystic development in the cord.
 Isolated from the patient’s bone
marrow the day before the surgery, a portion of the stem cells were
injected into the cystic cavity during surgery and the rest infused
intravenously. These patients were compared to 18 control patients with
SCI, who received the surgery only. Changes in motor function,
sensation, ability to carry out “activities of daily living,” and
spasticity were evaluated on average 9 months after surgery. Significant
improvements were noted in 12 of the 18 stem-cell-treated patients but
only 5 of the 18 controls. Isolated from the patient’s bone
marrow the day before the surgery, a portion of the stem cells were
injected into the cystic cavity during surgery and the rest infused
intravenously. These patients were compared to 18 control patients with
SCI, who received the surgery only. Changes in motor function,
sensation, ability to carry out “activities of daily living,” and
spasticity were evaluated on average 9 months after surgery. Significant
improvements were noted in 12 of the 18 stem-cell-treated patients but
only 5 of the 18 controls.
ASIA - CHINA, KOREA, & JAPAN
1) Dr. K-S Kang
et al. (South Korea) injected stems cells isolated from
umbilical cord blood (UCB) into the injury area of a 37-year old woman who
had sustained a T-10 complete injury 19 years earlier from a fall (Cytotherapy,
7(4), 2005). Unlike their embryonic counterparts, umbilical stem cells are
not controversial. They also have less rejection potential than most other
allogeneic donor tissue except embryonic tissue; i.e., some, but not
strict, matching between donor and recipient is needed.
In this case, human UCB was obtained from the Seoul
Cord Blood Bank, and the UCB cells isolated within 24 hours and, in turn,
cultured in media. The investigators indicated that when grown in a
neurogenic medium, the cells demonstrated features characteristic of
neurons and neuronal support cells (i.e., glia).
With this patient, after a laminectomy, one
milliliter containing one-million cells was injected “into the
subarachinoid space of the most distal part of the normal spinal cord.” An
additional one million stem cells were injected “diffusely into the
intradural and extradural space of the injured cord.”
The investigators reported that the patient regained
additional lower-limb function within 41 days of the transplantation,
including, according to other press reports, some walker-assisted
ambulatory ability. Various electrophysiological measurements supported
these observations. The investigators suspected that injecting the cells
directly into the spinal cord is more effective than infusing them into
the fluid surrounding the cord. They do not exclude the possibility that
functional improvement was due to laminectomy-related, spinal-cord
decompression.
Unfortunately, according to more recent press
reports, after her a second stem-cell treatment, her condition greatly
deteriorated. She is now unable to sit erect for long time periods and
spends most of her day in bed. According to her, “the improvements
disappeared quickly. I underwent another treatment, and this is the
result. I was unable to move and suffered from extreme pain.”
Doctors suggested she contracted an infection the
second time due to either procedural aspects or bacterial contamination of
the transplanted cells. As a result, the surrounding tissues have
hardened.
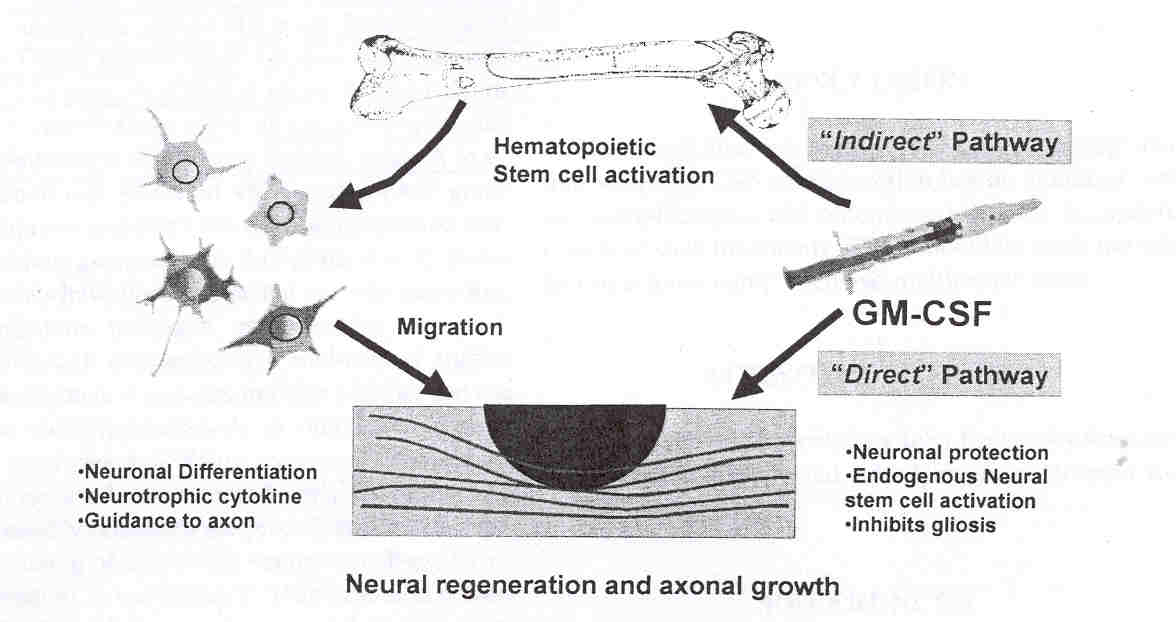
2) Dr. Yoon Ha
et al (South Korea) has transplanted bone-marrow cells (BMCs) into the
injury site of patients with acute SCI (7-14 days post injury) in
conjunction with granulocyte macrophage-colony stimulating factor (GMCSF),
a factor that stimulates stem-cell production. The bone-marrow cells
were aspira ted
from the patients’ iliac (i.e., hip) bone and further processed. Because
these autologous cells are isolated from the patient, there is no
rejection potential. After a laminectomy from one vertebra above to one
below the contusion site, a total of 1.8 milliliters of bone-marrow cell
paste were injected into six points near the injury site. ted
from the patients’ iliac (i.e., hip) bone and further processed. Because
these autologous cells are isolated from the patient, there is no
rejection potential. After a laminectomy from one vertebra above to one
below the contusion site, a total of 1.8 milliliters of bone-marrow cell
paste were injected into six points near the injury site.
All patients were men, ranging in age from 17 to 51
years. Five and one had cervical and thoracic injuries, respectively,
and all had ASIA-A complete injuries. Five received both bone-marrow
cells and GMCSF, and one received only GMCSF.
GMCSF was subcutaneously injected for first five
days of each month over five months. In addition to stimulating
bone-marrow stem-cell proliferation, animal models suggest that it may
also 1) activate macrophages (immune cells) to remove myelin debris that
inhibit axonal regeneration, and 2) inhibit post-injury cell death
through a process called apoptosis.
Although sensory improvements were noticed
immediately after the procedure, sacral-region sensory recovery and
significant motor improvements were observed three weeks to seven months
afterwards. Four patients, including the one that received only GMCSF,
improved from ASIA-A complete to ASIA-C incomplete injuries, one from
ASIA-A to B, and one remained at ASIA-A. MRI assessments 4-6 months
after injury showed slight enhancement.
Other than GMCSF-associated fever, the
investigators concluded that this BMC-transplantation procedure has no
serious complications, the study’s goal. Because this intervention and
follow-up assessments were performed during a period relatively soon
after injury in which some functional improvement is not uncommon, the
investigators were careful to avoid conclusions concerning overall
efficacy; however, they did quote studies indicating that only a
relatively small number (~6%) of patients improve from ASIA-A complete
to ASIA-B incomplete injuries.
3) Dr. Yongfu
Zhang and colleagues (China) have transplanted
autologous (i.e., isolated from the patient) bone-marrow stem cells into
90 patients with both acute and chronic SCI (1st International
SCI Treatments & Trials Symposium, Hong Kong, December 2005). Of these
patients, 10 had cervical injuries, 62 thoracic injuries, and 18 lumbar
injuries. The elapsed time from injury ranged from three days to six
years. “The injection site was in the upper and lower area between injury
and normal spinal cord.”
Thirty-three and 11 patients had improved sensory and
muscular ability, respectively after cell transplantation as measured by
Frankel assessments (which evolved into today’s ASIA standards). All
patients with clinical improvements sustained their injuries within a year
of the transplantation procedure. Treatment sooner after injury was
associated with better outcomes. The investigators suggested that the
bone-marrow stem cells improved blood circulation and inhibited glial scar
formation at the injury site.
4)
In 2008, Dr. Fukuki Saito et al (Japan)
reported the treatment of an acutely injured patient with autologous,
bone-marrow stem cells. A 35-year-old male, the patient sustained a
cervical C4-5 complete injury from a fall at a construction site. Three
days after injury, stem-cell-containing, bone-marrow tissue was
collected from the patient’s ilium (i.e., pelvis’ largest bone), and the
stem cells grown and amplified in culture for 10 days.
 Thirteen
days after injury, 31-million stem cells suspend in about two
milliliters of saline were transplanted into the cerebrospinal fluid via
lumbar puncture. Motor and sensory improvements were noted one and three
months after transplantation. Afterwards, little further improvement was
observed. Because some improvement is not uncommon in this post-injury
phase, it is difficult to ascertain how much of the restored function is
attributable to the stem cells and how much would have accrued anyway. Thirteen
days after injury, 31-million stem cells suspend in about two
milliliters of saline were transplanted into the cerebrospinal fluid via
lumbar puncture. Motor and sensory improvements were noted one and three
months after transplantation. Afterwards, little further improvement was
observed. Because some improvement is not uncommon in this post-injury
phase, it is difficult to ascertain how much of the restored function is
attributable to the stem cells and how much would have accrued anyway.
In 2012, Saito’s investigative team reported safety
and feasibility results of treating five patients with cervical injuries
with autologous bone-marrow-derived stem cells. The patients were all
men with age ranging from 23 to 59 years. Four sustained injuries from
falls and one from a traffic accident. Bone marrow was isolated from the
iliac crest within 72 hours of injury at the time when the patients were
undergoing surgery for spinal stabilization, a procedure which required
the isolation of an iliac bone segment. Stem cells were isolated from
the bone marrow and cultured. The cells were intrathecally transplanted
back into the patient by lumbar puncture within three weeks of injury.
Patients were followed for one to four years. During this period, no
adverse responses due to cell transplantation were observed. The
investigators concluded the procedure was safe. Although it is difficult
to attribute to the transplantation procedure due to the nature of the
study, significant functional recovery was observed in several
patients.
5) Beike
Biotechnology Company (China) was founded in 2005 with funding
from Beijing University, Hong Kong University of Science and Technology,
and Shenzhen City (near Hong Kong), and nurtured with Chinese government
grants. The company has established collaborations with 60+
scientists at leading Chinese universities. Building upon a base of
research starting a decade ago, Beike-affiliated doctors treated their
first patient in 2001; and in several years, had treated hundreds with a
variety of disorders. As confidence grew, they established Beike to
treat patients with stem cells on a commercial scale.
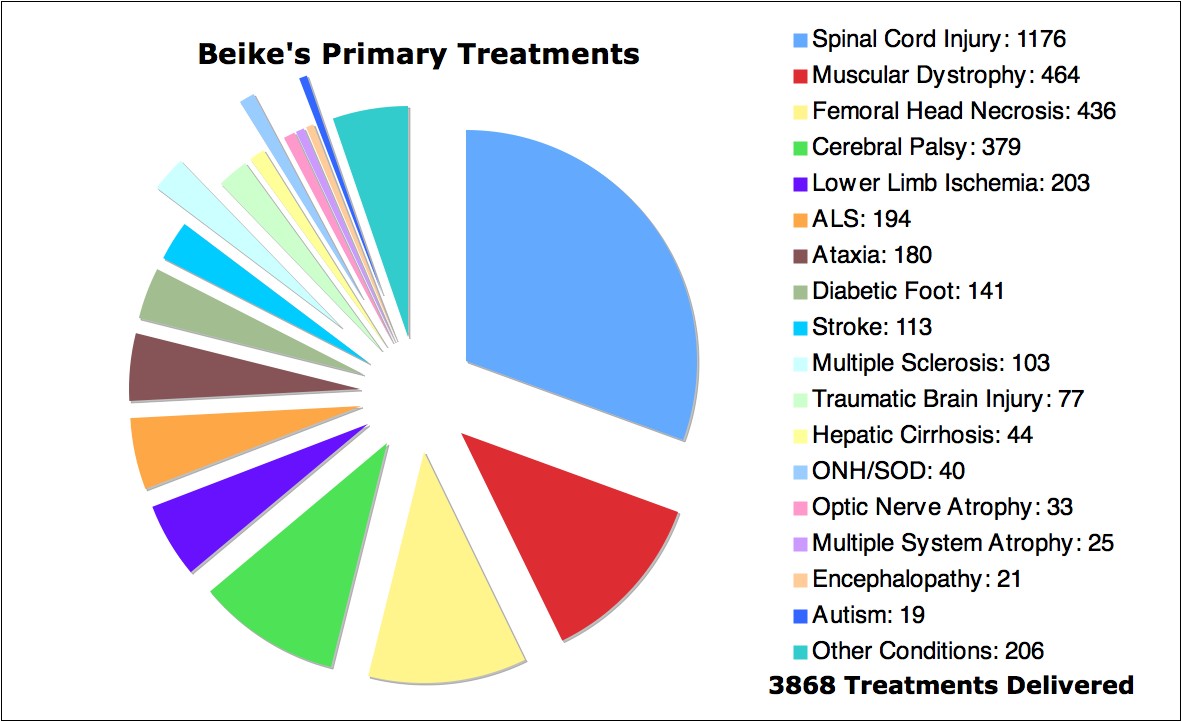
By the end of 2008, they had treated
~3,900 patients at about 30 clinics in China and one in Thailand, about
800 of which came from 35 other countries. Over a third of the patients
had spinal-cord dysfunction, including SCI (1176), MS (103), and ALS
(194); and 77 had traumatic brain injury.

Technically, however, Beike does not treat
patients. Through their 18 laboratories located throughout China, the
company provides stem cells to collaborating hospitals. It is the
hospitals who have been granted the authority from the China Ministry of
Health to treat patients in Beike-established clinics. Although many
Chinese hospitals provide stem-cell therapy, Beike is the country’s
largest stem-cell source. To make the therapy more internationally
accessible, Beike will be establishing laboratories and treatment
centers in India, Europe, Middle East, and either Panama or Mexico.
Beike transplants a variety of stem cells by
different routes. Frequently, the company uses umbilical cord stem
cells, in part, because cord blood is commonly collected after birth by
Chinese blood banks. Beike also transplants stem-cells obtained from the
patient’s bone marrow. Cells are usually transplanted either
intravenously or by lumbar puncture, the latter which introduces the
cells directly into the CNS. Occasionally, cells have been implanted
directly into the spinal cord.
After testing for diseases, the cord blood is
transferred from the blood bank to a Beike laboratory and retested. Stem
cells are separated from blood cells and platelets through
centrifugation and then cultured in a media containing growth factors,
which enhance rejuvenation potential. The growth media is washed away,
leaving the desired stem cells. To ensure viability, all stem-cell
preparations are fresh and not frozen for later use.
Typically, patients receive 4-7 stem-cell
injections over a 25-35 day period. This treatment regimen is
supplemented with individually tailored, rehabilitation programs.
Many Beike-treated patients with SCI have regained
life-enhancing benefits, ranging from the subtle to fairly dramatic.
Although improvements with some disorders may fade over time, SCI gains
seem to be enduring. Consistent with more long-term physiological
mechanisms, benefits often slowly kick-in after stem-cell treatment and
returning home.
In general, Beike prefers treating individuals with
incomplete injuries. According to Beike founder Dr. Sean Hu: “Spinal
cord injuries are very interesting as they seem to go against the
earlier-is-better rule. We have found that some of our best cases have
been the patients who have had injuries for over 20 years…We have
discovered a better response in these patients compared to those with an
injury sooner than six months. As a result… we generally do not allow
the hospitals to accept patients whose injuries have happened in the
last six months.”
Study: Beike scientists have evaluated the
effects of treating 500 patients with umbilical-cord-blood stem cells
(465 completed the study). Patients were 18-65 years old, 78% were men,
and all had been injured 1-10 years before treatment (C4-T10 injuries).
Patients received 4-5 intrathecal injections containing 10-30 million
stem cells at one-week intervals and followed for a year using several
evaluation parameters, including commonly used ASIA assessments
(American Spinal Injury Association) for motor function and sensation.
Statistically significant, modest improvements were documented which
continued after the final injection. No serious side effects observed.
Many patient experiences are posted at
www.stemcellschina.com, including before-and-after-video
documentation, including the following case. The patient was a
30-year-old Romanian male, who sustained a C5-6 incomplete injury in
1995 from a diving accident. After three sets of stem-cell injections,
he posted the following [English edited]:
“My hand movements are
much better. I have more power in my hands and body, and new sensations
all the way down to my feet, almost 90% … I feel my hands 100% now.”
“I’ve started to move my
fingers a little and can feel pain in my first two fingers. I also can
feel a lot of heat in my legs, and…can move my feet, but only 1-2 times.
Now, I can contract my stomach muscles. I can stay on my feet 30-50
minutes, but with assistance and support on my knees. I have more
stability than before, and when I’m on my feet I can move my hands and
body more because my abdominal and back muscles are stronger.”
When lying in bed, I can move my feet a little … I can hold my urine for
5-10 minutes before I have to go. My sensation is much improved; I can
feel better my legs and all my body for temperature, as well as pain and
touch (skin) sensation…My stability is much better than before, I can
sit on the bed without support, and if my mother pushes my legs forward,
I can move them back. So, now I have started to move my legs; even if it
is a little, it’s a start. My triceps have started to work too.”
6)
Doctors at Tiantan Puhua Hospital, Beijing,
China have established a stem-cell center for treating a
variety of neurological disorders, including SCI. Stem cells from
various sources have been transplanted into the patients via a number of
routes. The center’s program has also incorporated a “self stem-cell
activation and proliferation” component in which an individually
customized cocktail of “neurotrophic medicine” is intravenously
administered daily to the patient. It is claimed that this cocktail
stimulates the patient’s own stem cells to differentiate into nerve
precursor cells and migrate to where they are needed. The treatment
experiences of several patients are posted on the center’s website
www.stemcellspuhua.com.
The center has reported transplanting bone-marrow-derived stem cells into patients with
SCI, five with chronic injuries sustained at least a
year before treatment. Because the cells are isolated from the
patient’s own bone marrow (i.e.,autologous), they will not be
immunologically rejected when transplanted back into the patient.
Considering the injury-site “glial” scar as a barrier to regenerating
neurons, the doctors ablate (remove) the scar by “medicine” before the
cells are transplanted. The cells are grown and amplified in culture for
about 3-4 weeks to obtain about 4,000,000 cells, which are then
transplanted back into the patient in 3-4 injections spaced two weeks a
part. The cells are either implanted into the patient’s spinal cord
fluid by lumbar puncture or surgically implanted directly into the
injured cord.
7)
As discussed elsewhere, a network of Chinese
SCI centers have been established to
carry out clinical trials on promising therapies. Initial network
studies focus on the use of lithium and umbilical-cord-blood-derived
stem cells (see “Pharmaceutical Approaches”). These two approaches are
being considered together because evidence suggests that lithium
stimulates these cells to proliferate and to generate beneficial
neuronal growth factors.
After evaluating lithium’s safety in individuals
with SCI, a phase-2 trial was initiated assessing the effects of
implanting increasing amounts of umbilical-cord-blood-derived stem cells
into the cord above and below the injury site in individuals with
chronic SCI combined with lithium treatment. Finally, in a phase-3
trial, the investigators intend to implant the stem cells into 400
subjects randomized to receive either placebo or lithium for six weeks.
Similar studies are being planned in the United States and India.
ASIA - INDIA & OTHER
1) Dr. Geeta
Shroff (New Delhi, India) has used human embryonic stem cells
(ESC) to treat over 300 patients, including 70 with SCI. Impressive
results have accrued, and especially important given the theoretical
risks of ESC, no adverse side effects have occurred.

All cells that have been transplanted into the many
patients numerous times were derived from a single, surplus fertilized
egg from Shroff’s in-vitro-fertilization (IVF) program. Developed with
donor permission, this fertilized egg would have been disposed of under
normal circumstances. Clearly, Shroff’s success was facilitated by her
extensive experience working with embryonic cells as a fertility doctor.
Her 70% success-rate in making women pregnant through IVF is quite high
compared with most other programs. Apparently, the skills she acquired
in developing healthy embryos translated well into the creation of
robustly therapeutic stem cells. Her cells are prepared with “Good
Manufacturing Practice (GMP)” and “Good Laboratory Practice (GLP)”
quality-control standards.
Shroff’s key breakthrough is that she has grown ESC
without using any animal products, including animal feeder cells often
used by other researchers. By keeping the cells purely “human” in
nature, she makes them more amenable to transplantation. The cells from
her “mother culture” are further adapted or primed to create daughter
cultures targeting specific disorders. Hence, a more specialized cell
line will be used to treat individuals with SCI, stroke, diabetes, etc.
According to Shroff, the transplanted cells will home into the tissue
where they are needed. Thus, even when introduced by more remote
intravenous or intramuscular routes, the cells’ physiological affinity
for the target tissue will cause them to migrate where they are needed.
Shroff’s ESC use is allowed under Indian stem-cell
guidelines if the condition or disorder is considered incurable. Given
the snail-pace development of real-world stem-cell therapies in many
countries, these are insightful guidelines.
Countering criticism she’s using the vulnerable and
disadvantaged as guinea pigs, Shroff notes that 30% of her patients are
physicians or have family members who are physicians. In other words,
highly educated medical professionals who appreciate underlying issues
have chosen to avail themselves of the treatment. In addition, a number
of senior government officials have been treated and, based on their
comments to me, are delighted with the benefits. Documenting interest in
her program at the highest levels, Shroff has briefed the Indian
President and Prime Minister. Finally, showing that her program is more
than just a profit-making venture, many of her indigent patients have
been treated without charge.
Shroff has treated over 100 persons with SCI.
Although she believes that treatment would be optimal when started close
to injury, most of her patients have been injured for at least a year.
Basically, she decided not to treat the more acutely injured patients
because critics would dismiss improvements as something that would have
occurred anyway during a period in which functional gain is not
uncommon.
Patients often visit the clinic several times for a
series of transplantations. The cells are introduced through a variety
of routes, including intravenous or intramuscularly injections, and more
infrequent intrathecal transplantations directly into the spinal-cord
region. The number of transplanted cells increases over time. All
patients are carefully followed to document progress.
One of Shroff’s more well-known patients was Ajit
Jogi, a 60-year-old Indian parliament member and former chief minister
of an Indian state, who sustained a cervical injury from a 2004 auto
accident. After injury, Jogi was unable to sit up and had difficulty
breathing and even writing. Since treatment, he can walk about 10 steps
with braces, has regained significant bowel and bladder function, has
full sensation down to his toes, and, with the renewed, very-evident
energy has resumed a politician’s busy life style.
2)
Dr. Satish Totey
and colleagues (India) initiated a pilot study evaluating the
effectiveness of transplanting bone-marrow-derived, mesenchymal stem
cells isolated from the patient (i.e., autologous) back into the
patient. The cells were extracted from the hip bone and cultured several
weeks before being transplanted back into the patient. Twenty-two
subjects with complete (ASIA A), C4-T10 injuries sustained within the
previous half year were to be recruited into the study. Approximately,
one-million stem cells per kilogram of body weight were injected by
relatively non-invasive lumbar puncture into the spinal-cord fluid. To
evaluate potential improvements or changes, various
electrophysiological, imaging, and clinical assessments were carried out
before and three months after transplantation. Twenty-two
subjects with complete (ASIA A), C4-T10 injuries sustained within the
previous half year were to be recruited into the study. Approximately,
one-million stem cells per kilogram of body weight were injected by
relatively non-invasive lumbar puncture into the spinal-cord fluid. To
evaluate potential improvements or changes, various
electrophysiological, imaging, and clinical assessments were carried out
before and three months after transplantation.
At the time this information was collected, 12
subjects had been recruited, of whom one had completed the three-month
assessments. This individual, a 32-year-old male, initially received two
stem-cell transplantations nearly two weeks apart. In addition to
improvements noted by various electrophysiological assessments, the
patient reported improved bowel-and-bladder function; increased
sensation; improved muscle function and strength, including some
ambulation and toe wiggling, and overall enhanced strength.
In 2009, Dr. Totey and his associates reported the
results of treating 30 patients with SCI with autologous,
bone-marrow-derived mesenchymal stem cells. All but three of the
patients were men, and age ranged from 21 to 56 years. Twenty had
injuries of between one-month and six-months duration, and 10 had
injuries of greater than six-months duration. Bone marrow was isolated
from the iliac crest of the pelvis bone and processed in culture to
obtain the stem cells. The cells were intrathecally reintroduced into
the patient by lumbar puncture.
Patients were evaluated using a variety of
assessments, including the ASIA scale (see appendix), a measurement of
patient independence and quality of life, and electrophysiological tests
for nerve conduction. At the time of publication, 3, 10, and 10 patients
had completed three years, two years, and one year of follow-up,
respectively. Five patients were lost to follow-up.
The results indicated that the procedure caused no
serious adverse effects. According to the investigators, two patients
“showed significant clinical and functional recovery… and the rest of
the patients have shown variable patterns of recovery,” including
bladder function. One year after transplantation, improvements were
noted in patient independence for those with thoracic injuries who had
been injured for less than six months at the time of transplantation.
However, no such change was noted for those with cervical injuries and
those who had been injured more than six months at transplantation.
3) Dr. R.
Ravi Kumar and colleagues (India) have transplanted
autologous (i.e., obtained from the patient) stem cells into over 120
patients with SCI. Stem-cell preparation was done in
association with the Nichi-In Center for Regenerative Medicine, a
Japanese laboratory located in India that specializes in the preparation
of autologous - no-rejection - stem cells. Stem cells were
extracted from 100 ml of bone marrow obtained from the patient. The
concentrated preparation, containing about 2-4 million cells, was
injected into the lumbar spinal fluid (i.e., intrathecal).
According to presentations at 2007 stem-cell
meetings, 120 patients who received stem cells in this fashion were
followed for six months. Of these patients, 85 were male and 35 female;
age ranged from 8-55 years; and time lapsing from injury varied from
three months to 11 years. Nine patients had cervical injuries, 38 upper
thoracic (T1-T7) injuries, 60 lower thoracic (T7-T12), and 12 lumbar
injuries.
Six months after transplantation, 12 and 8 patients
improved at least two or one grade(s) of motor power, respectively
(greater improvement noted for lower-level injuries); three could walk
independently; 14 had sensory improvement or pain reduction; and 18 had
improved bladder control. No significant adverse side effects were
noted.
In 2009, the investigators reported the results of
treating 297 patients with autologous, bone-marrow-derived stem cells
obtained from the patient’s iliac crest of the pelvis (8). Of these
patients, 215 had traumatic paraplegia, 49 had traumatic quadriplegia,
and 33 had various other forms of spinal cord dysfunction. The isolated
cells were transplanted back into the patient through a lumbar puncture
(i.e., into the cerebrospinal fluid). The patients were followed in
three-month intervals for cumulative periods ranging from 18.4 to 20.5
months. The investigators concluded that the transplantation of
autologous, bone-marrow-derived cells through a lumbar puncture is safe,
and that one third of the patients had “perceptible improvements in
neurological status.” Improvements appeared to be greater for more
recently injured individuals.
4) Dr.
Adeeb Al-Zoubi and colleagues (Jordan) reported
their experience transplanting purified stem cells into eight patients
(6 males and 2 females) with complete thoracic level injuries. The stem
cells were isolated from the blood of the patient (i.e., autologous)
after treatment with granulocytic-colony-stimulating factor, a drug that
promotes stem-cell production. On average, 51-million stem cells were
implanted into the injury site’s cyst cavity or subarachinoid space (a
space between the spinal-cord membranes filled with cerebrospinal
fluid). After nine months of patient follow up, no adverse side effects
were observed. Four patients demonstrated sensory improvement and two
motor-function improvement.
In 2010, Al-Zoubi discussed the results of
transplanting bone-marrow-derived, purified stem cells into ~50
patients with SCI. Isolated from the patient’s bone marrow – not the
blood as above - these cells were reintroduced into the patient’s spinal
cord. Although some improvements were noted, he believed the results to
be “suboptimal.” As such, Al-Zoubi is researching ways to better
prepare, process, and differentiate these and other bone-marrow-derived
cells into more neurologically oriented stem cells with, in turn, a
greater potential to treat SCI.
5) Dr. Haluk
Deda and colleagues (Turkey) have transplanted autologous,
bone-marrow-derived stem cells into nine patients (5 males and 4
females) with ASIA-A complete injuries. Age ranged from 17 to 40 years,
and the time lapsing from injury varied from two to 17 years. Six and
three patients had cervical and thoracic injuries, respectively.
Approximately 100-150 milliliters of stem-cell-endowed bone marrow was
aspirated from the pelvis’ iliac crest, sent to a company in Michigan
for stem-cell processing and purification, and returned to the hospital
for implantation. The injured spinal cord was exposed by a laminectomy
and carefully cutting of the covering membranes. Any bone fragments and
adhesions around the injury area were removed. Stem cells were implanted
by several mechanisms, including: 1) multiple injections directly into
the cord at different depths, 2) covering the exposed cord by a
stem-cell-containing gel foam, 3) injection into the subarachnoid space
(i.e., the space that contains cerebrospinal fluid) after membrane
closure, and 4) intravenous injection. Functional improvements were
noted in all patients as early as three weeks after the procedure. A
year after transplantation, seven of the nine patients had improved from
ASIA-A complete injuries to ASIA-C incomplete injuries (i.e., regaining
some motor and sensory function), and two had improve to ASIA-B
incomplete injuries (i.e., some sensory recovery).
6) Dr.
Himanshu Bansal (India) has used several procedures in an
effort to restore some post-injury function, including, as discussed
here, stem-cell transplantation and, as reviewed later, omental
transposition.  In
preliminary investigations, Bansal has transplanted bone-marrow-derived
stem cells into 11 patients with motor-sensory complete injuries (i.e.,
ASIA-A) sustained at least a year earlier from contusion or laceration.
Nine possessed cervical injuries and two thoracic injuries, and all
except one were men. Although most were younger than 30, age ranged from
20 to 52. In
preliminary investigations, Bansal has transplanted bone-marrow-derived
stem cells into 11 patients with motor-sensory complete injuries (i.e.,
ASIA-A) sustained at least a year earlier from contusion or laceration.
Nine possessed cervical injuries and two thoracic injuries, and all
except one were men. Although most were younger than 30, age ranged from
20 to 52.
The stem cells were obtained by aspirating ~120
milliliters of bone marrow from the patient’s iliac crest, a bone-marrow
abundant area of the pelvis bone, and then obtaining a stem-cell rich
concentrate by centrifugation. To maintain their fundamental nature, as
well as the presence of regenerative-enhancing growth factors, no
further physical, chemical, or biological processing of the cells was
carried out before transplantation.
In some patients,
cells were directly injected into the area around the spinal-cord injury
site and, in other cases, into the cord’s surrounding intrathecal space.
Although the post-transplantation follow-up time period has been
limited, results suggest that some improvement accrued for the six
patients who had cells directly implanted into their injured cords.
Bansal noted that two of them “had a 100% improvement in bladder
control, one had good improvement in motor scores, and one had improved
coordination and walking ability with sensory improvement.” With higher
level injuries, he observed recovery of trunk control and decreases in
spasticity. Because the five patients who received stem cells
intrathecally had little improvement, Bansal no longer uses this route
of administration. He believes post-transplantation aggressive physical
rehabilitation is especially important in promoting the development of
function-restoring nervous-system connections.
7) Dr.
Sunil Waghmare and colleagues at the Spectrum Cell Clinic
(India) have used either umbilical-cord-blood or autologous bone-marrow
stem cells to treat a wide variety of disorders, including SCI. In the
case of SCI, the cells have been implanted into patients by several
routes, including 1) via a blood vessel that supplies the front area of
the spinal cord (anterior spinal artery), 2) intrathecally into the
space surrounding the cord, and 3) directly into the injury-site area.
In general, the clinic prefers employing less invasive techniques using
local anesthesia
At the time of this report, the clinic had treated
about 30 individuals with varying degrees of injury completeness as
determined by the commonly used ASIA impairment scale (see appendix).
Waghmare notes that in the case of incomplete injuries, the therapeutic
response is ~75-80% with improvement of more than two grades on the ASIA
scale. With complete injuries, treatment often results in a one-grade
improvement. In an anecdotal case described on the clinic’s website, a
42-year-old male, who had sustained a C5-6 incomplete injury 13 years
earlier, reported significant functional improvements after three
stem-cell treatments, including 1) regaining bowel and bladder control,
2) increasing muscle bulk and coordination, and 3) a lessening of
spasticity.
8)
Dr. Alok Sharma and associates at the
NeuroGen Brain and Spine Institute (India) have transplanted
bone-marrow-derived, autologous (i.e., from the patient stem cells into
many individuals with diverse neurological disorders, including SCI.
 Routinely,
several days after treatment with a drug that stimulates stem-cell
production, bone marrow is aspirated from patient’s iliac crest bone of
the pelvis area. The stem cells are then separated from the bone marrow
and stem cells intrathecally transplanted back into the space
surrounding the patient’s spinal cord. To maximize post-transplantation
functional return after transplantation, patients are encouraged to
undertake physical rehabilitation either at the clinic or at home.
According to the NeuroGen website, patients have regained life-enhancing
function relatively soon after treatment. Routinely,
several days after treatment with a drug that stimulates stem-cell
production, bone marrow is aspirated from patient’s iliac crest bone of
the pelvis area. The stem cells are then separated from the bone marrow
and stem cells intrathecally transplanted back into the space
surrounding the patient’s spinal cord. To maximize post-transplantation
functional return after transplantation, patients are encouraged to
undertake physical rehabilitation either at the clinic or at home.
According to the NeuroGen website, patients have regained life-enhancing
function relatively soon after treatment.
9) In 2011,
Dr. Ayhan Attar
and colleagues (Turkey) reported the results of treating two men
and two women with autologous (i.e., from the patient)
bone-marrow-derived stem cells. Patient age ranged from 19 to 25, and
all had ASIA-A complete injuries (see appendix) sustained approximately
one month before transplantation. Bone marrow was obtained from the
patient’s pelvis bone ilium, which, in turn, was processed and the
resulting stem cells reintroduced into the spinal-cord injury lesion.
All patients underwent six-months of rehabilitation and were
periodically followed with a variety of assessments. At the end of one
year, two patients had improved to ASIA-C (some sensory and motor
recovery), one had improved to ASIA-B (some sensory improvement), and
one had not demonstrated any improvement.
AFRICA
1)
Dr. Nirmeen Kishk and
colleagues (Egypt) transplanted autologous (i.e., isolated from the
patient) bone-marrow-derived mesenchymal stem cells into 43 subjects
with chronic SCI. Mesenchymal stem cells have the potential to 1)
differentiate into a variety of tissue types (see figure) depending upon
the unique signals from the local physiological environmental, and 2)
detect and migrate toward injured tissues.
The treatment group was composed of 36 men and
seven women with an average age of 32 and average time lapsing since
injury of 3.6 years. Eighty-six and 6% had thoracic and cervical
injuries, respectively, and 12 injuries were labeled complete and 31
incomplete as determined by MRI assessments (i.e., magnetic resonance
imaging). The treatment group was compared to a similarly composed
control group of individuals who had refused stem-cell transplantation.
Procedurally, 10-20 milliliters of bone marrow was
isolated from the patient’s pelvis’ iliac bone. After processing, the
mesenchymal stem cells were isolated and injected intrathecally into the
patient’s lumbar region (i.e., lumbar puncture) once a month for six
months. All subjects, including controls, participated in thrice weekly
rehabilitation sessions composed of a variety of training and
strengthening exercises.
Twelve months after completion of the six-month
stem-cell intervention, functional recovery was evaluated using a number
of assessments. Although stem-cell treated patients demonstrated slight
improvements in motor, bladder, and bowel function, overall, little
difference was observed between treated and control subjects.
Furthermore, any improvements were counterbalanced by a number of safety
concerns, including an increased incidence of both neuropathic pain and
spasticity, which was not observed in control subjects. The
investigators concluded that given adverse side effects, more controlled
studies should be carried out before these stem cells “should be offered
to patients.”
OTHER
1)
Advanced Cell Therapeutics
(ACT) According to the company’s website, ACT, registered in the Caribbean
Turks and Caicos with connections in South Africa, provides “access to
cord blood stem-cell therapy in locations where the treatment is
lawful...” According to ACT-generated resources, their cord-blood
stem-cell protocols have been used over 700 times for over 80
conditions, including SCI. There has been much adverse publicity
concerning ACT operations, and the true nature of the cells.
ACT claimed to have enhanced the therapeutic
effectiveness of their stem-cell preparations through a number of
procedures. First, white and red blood cells were removed, minimizing
rejection potential. Second, key CD133+ stem cells were amplified from
the normal 10% of cord-blood stem cells to an elevated 70-80% level.
These CD133+ as well as standard CD34+ cells are considered especially
powerful stem cells due to their enhanced ability to zero in on a target
tissue, differentiation, and engraftment. Third, ACT developed
procedures to differentiate cord-blood stem cells into more specialized
lines, such as neuronal stem cells for brain and spinal-cord
regeneration or pancreatic stem cells for diabetes. Finally, the company
supposedly developed freezing techniques that enhanced cell viability
after thawing.
ACT reported treating eight patients with chronic
SCI with cord-blood stem-cell preparations. Patient age range from 18 to
43; five and three had quadriplegia and paraplegia, respectively; and
most injuries were incomplete. About 1.5-million stem cells were
introduced into the patient by intravenous and/or subcutaneous
injection. After a relatively short follow-up period, most patients
reported some functional improvements, including increased sensation,
ambulatory ability, and bowel-and-bladder function.
TOP
|
| |
| |
|
| |
| |
|
| |
| |
|
|




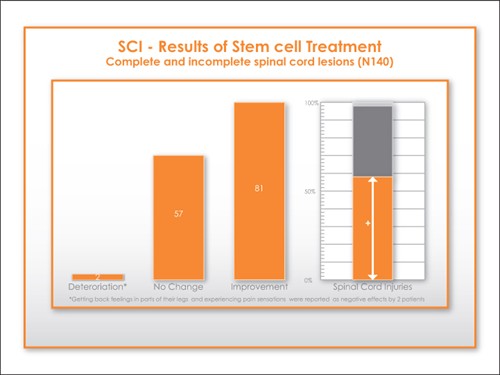
.jpg)
.jpg)