1) Dr. Carlos Lima (Portugal)
2) Dr. Hongyun Huang (China)
3) Dr. Alan MacKay-Sim
(Australia)
4) Dr. Tiansheng Sun (China)
5) Dr. Wlodzimierz
Jarmundowicz & Dr. Pawel Tabakow (Poland)
1) Dr. Carlos
Lima (deceased 2012) and colleagues (Lisbon, Portugal and other countries)
implant whole olfactory tissue obtained from the patient (i.e., no
immunological rejection) back into the injury site (click on
illustration)
(J
Spinal Cord Med 29(3), 2006).
 Lima believes that more than one cell type is needed to
maximize regeneration, including not
only OECs but also olfactory neurons in different developmental stages,
and precursor stem cells.
Lima believes that more than one cell type is needed to
maximize regeneration, including not
only OECs but also olfactory neurons in different developmental stages,
and precursor stem cells.
In Portugal, Lima's team has treated 120+ patients
from throughout the world, including from the USA (53), Portugal (21),
Italy (11), Canada (3), UK (3), and other countries (10). Fourteen
patients have also been treated in Columbia, seven in Greece, and six in
Saudi Arabia. In addition, new treatment centers are being planned in
Japan, India, and New Zealand (September 2006 update). Purportedly, many
of the patients have accrued significant benefit.

Lima’s work was
featured on an award-winning PBS documentary entitled “Miracle Cells.”
In 2005, the World Technology Network
named Lima as a finalist for a prestigious innovation award in health and
medicine.
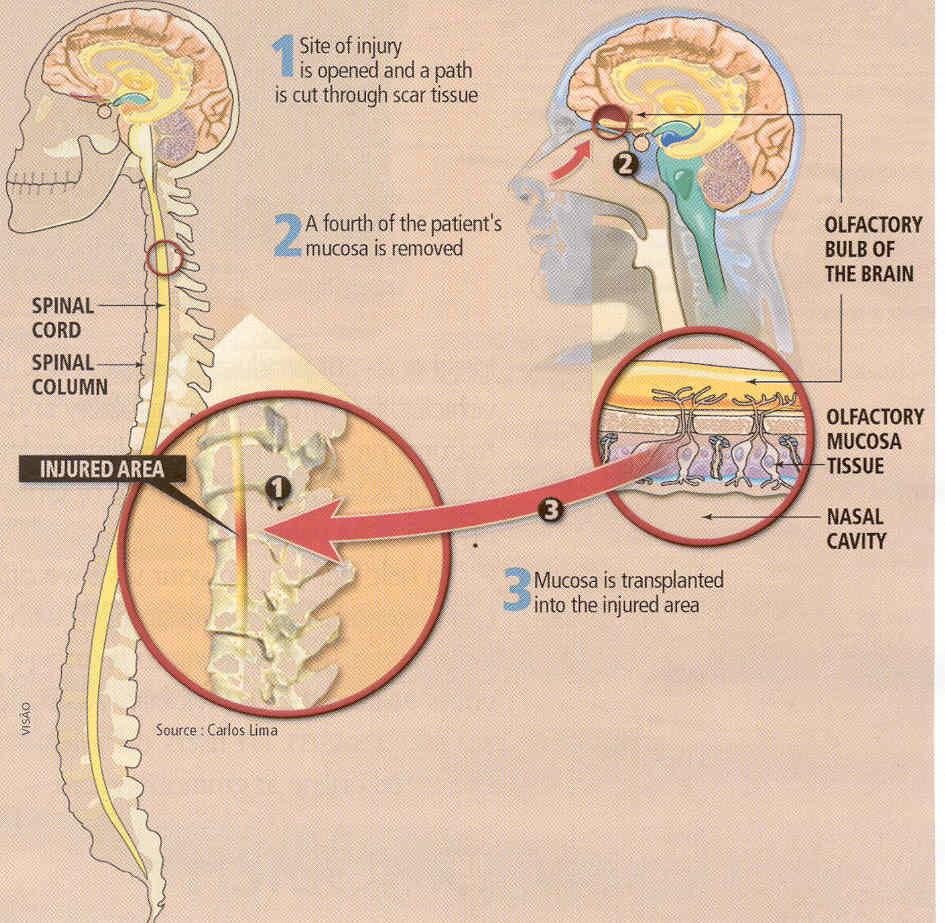
The surgery’s
critical procedure is the collection of about one fourth of the patient’s
olfactory tissue through unique procedures that maximize the harvesting of
that tissue and minimize the collection of closely associated nasal
respiratory tissue. Although Lima’s experience indicates that small
amounts of contaminating respiratory tissue are innocuous, it nevertheless
lacks olfactory tissue’s regenerative components. Because olfactory tissue
can diminish over time, patient age is important, and as a result, he
usually does not accept patients older than 40. Patients regain smelling
ability within several weeks.
The injury site
is exposed with a laminectomy and then myelotomy (cutting open the cord’s
membrane coverings). Although it is impossible to remove all of the scar
tissue at the injury site cavity, the scar’s top and bottom stumps are
taken off so that the cord is visible, and in between, holes are made in
the scar.
The isolated
olfactory tissue is dissected into small pieces while it is immersed in a
small amount of the patient’s cerebrospinal fluid. The pieces are then
implanted into the cavity. Lima estimates that a 1-cm2 cavity
filled by this tissue will contain approximately 400,000 stem cells and 4
million each of mature neurons, immature neurons, and other supporting
cells.
Lima believes
maximal restored function will require aggressive rehabilitation. To
separate the function-restoring effects of such physical rehabilitation
with the procedure itself, many of the more recent patients have been
required to initiate physical rehabilitation before the surgery and not
just afterwards.
For example, the Detroit
Medical School has developed an intense rehabilitation program that has
treated 34 patients who have undergone olfactory-tissue program.
A number of
articles published in professional journals have focused on Lima’s
procedures, including the following:
1) In 2006,
Lima’s team reported the results
of transplanting olfactory tissue into the injury site of seven patients
with SCI over the July 2001 to March 2003 period. These patients were
among the initial ones treated with Lima’s procedures.
Four patients
were men, and three were women. Their age ranged from 18 to 32 (average
23) years, and the time since injury varied from 0.5 to 6.5 years. The
spinal cord injury site ranged from the cervical C4 to thoracic T6
level. All patients had been injured from road accidents, except one who
was injured from a fall. Using the ASIA-impairment scale (American
Spinal Injury Association – see appendix),
in which grade A corresponds to a complete injury and grade E
corresponds to recovery, all patients had grade-A injuries before
transplantation. The length of the injury-site lesion ranged from one to
six centimeters (2.4 inches).
Post-procedure
magnetic resonance imaging (MRI) indicated a complete filling of the
lesion sites except for the patient with the largest, six-centimeter
lesion. Eighteen months after injury, all patients demonstrated varying
degrees of improvement in either sensation or motor function in
paralysis-affected muscles. Two improved from ASIA-grade-A (complete) to
ASIA-grade-C (incomplete) injuries. One patient lost some sensation but
gained motor function and believed that the trade-off was worth it.
Electrophysiological evaluations of nerve conduction indicated that
three patients could voluntary control muscles that they were unable to
do so before the procedure. One patient reported the return of bowel
control, and two patients recovered sufficient bladder sensation to
allow a discontinuation of catheterization.
Although the
procedure involved the removal of a portion of the subject’s olfactory
tissue for transplantation into the injury site, all subjects eventually
recovered normal smelling capability within three months.
2) In a 2009 article,
Lima’s team reported the results of a more comprehensive study which
transplanted olfactory tissue into 20 patients followed by extended,
aggressive physical rehabilitation. Recruited between April 2003 and
December 2006, these patients were different from the ones recruited in
the previous study. The investigators hypothesized that three treatment
components are critical for functional improvement: 1) transplanting
stem-cell-containing olfactory-tissue (i.e., not just olfactory
ensheathing cells), 2) cleaning out injury-site scar tissue to make room
for transplanted tissue and to remove regeneration barriers, and 3)
intense rehabilitation.
Patients were
required to carry out extensive physical rehabilitation both before and
after transplantation. Because there is an understandable desire to
maximize the functional benefits after any cell-transplantation
procedure, subjects tend to rehabilitate much more aggressively after
transplantation than before. By so doing, it becomes difficult to
attribute any restored function to merely the transplantation. In other
words, improvement may be just due to a now highly motivated individual
doing a lot of physical rehabilitation.
Subject
Characteristics: Seventeen men and three women were enrolled into
the study. Age ranged from 19 to 37 (average 30) years. The time lapsing
from injury to transplantation varied from 1.5 to ~16 years; in other
word, all subjects had chronic injuries. With such injuries, relatively
little additional recovery is spontaneously expected, and, as such, any
improvement is most likely due to the intervention. Injuries were
sustained from traffic (14), sports (4), and work accidents (2).
Thirteen subjects had cervical injuries ranging from the C4 to C8 level,
and seven had thoracic injuries ranging from the T5 to T12 level.
Fifteen subjects
had grade A (sensory and motor complete) and five grade B (motor
complete) injuries at the time of transplantation. Because the
injury-site scar tissue is removed as a part of the procedure, all
lesions had to be less than three centimeters (~1.2 inches) in length
for cervical injuries and four centimeters for thoracic injuries.
Physical
Rehabilitation: Subjects
averaged 32-hours per week rehabilitation for 35 weeks before
transplantation; and postoperative rehabilitation averaged 33 hours per
week for 92 weeks. Rehabilitation was undertaken at three centers, two
in Portugal and one in Italy. One center used robotic
bodyweight-supported treadmill training (see discussion under “Treadmill
Rehabilitation Programs”), and the other used an assisted over-ground
walking training with weight bearing on the hips and feet to promote
sensory and muscle-movement feedback. Results indicated that the latter
approach was much more effective in promoting functional improvement
after transplantation. The investigators now believe that this method
allows the movement freedom to promote the development of new movement
patterns that may enhance functional connections.
Results:
Various functional status assessments were carried out before
transplantation (i.e., baseline) and periodically afterwards. Average
duration of follow-up was 28 months.
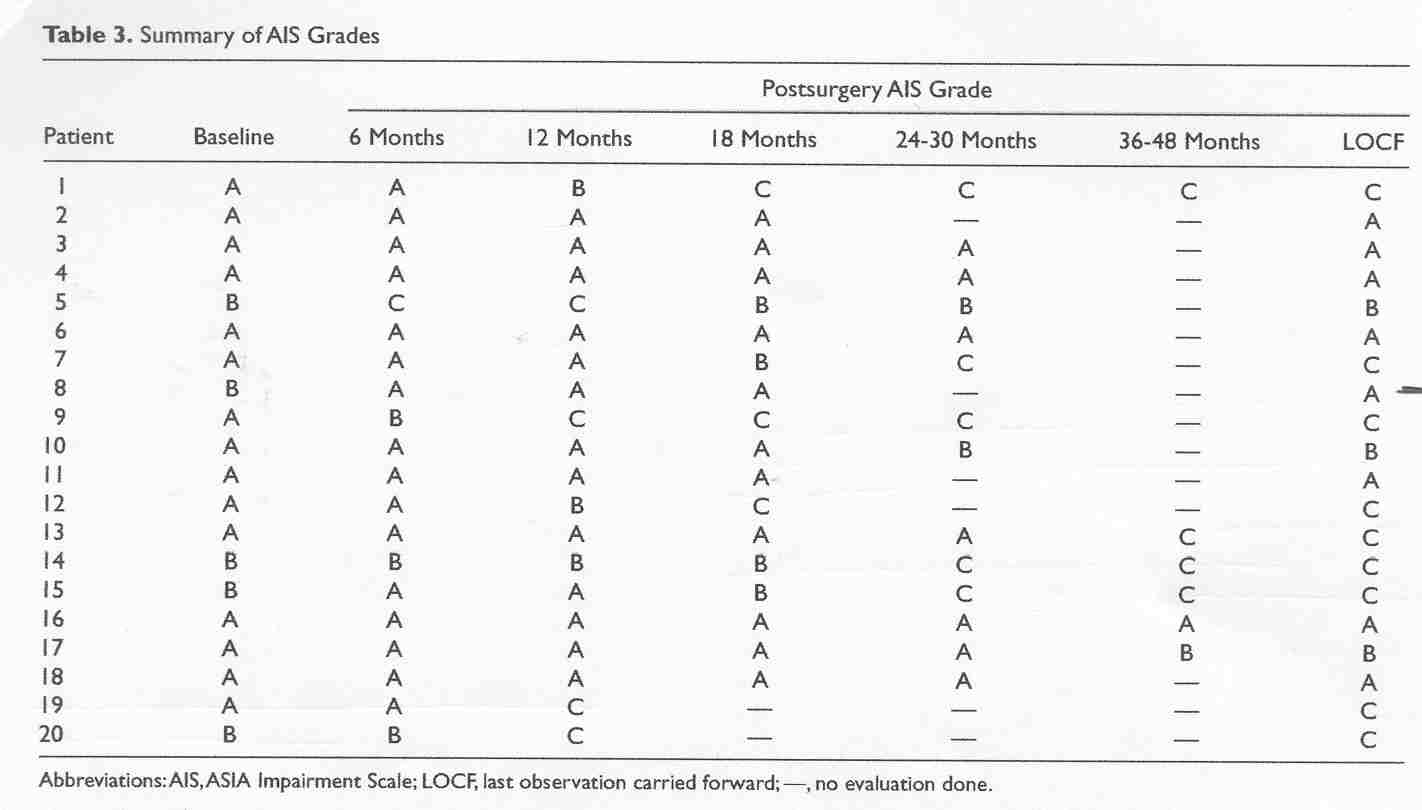
A) Impairment
Scales: Using
ASIA-impairment evaluations, 11
of the 20 subjects improved one grade or more. Specifically, six
improved from grade A (complete injury) to grade C (regaining some
sensation and motor function), three from grade B to C, and two from
grade A to B (i.e., recovery of some sensation). Although there w as
considerable patient variability,
motor-function, light-touch, and
pin-prick scores all improved on average.
as
considerable patient variability,
motor-function, light-touch, and
pin-prick scores all improved on average.
B) Walking:
Thirteen subjects from two of the three study centers were evaluated for
ambulatory improvements using the “Walking Index for Spinal Cord Injury”
(WISCI), a measurement which assesses the amount of assistance required
for ambulation. All 13 demonstrated some improvement using this
evaluation, one progressing from no mobility to walking 10 meters with
braces and crutches.
C) Functional
Independence: The same 13 subjects were also evaluated for their
ability to carry out various activities of daily living and self care
(e.g., eating, grooming, bathing, etc) by using of the FIM scale
(Functional Independence Measure). The scale is a predictor of the
amount of assistance or adaptive equipment an individual may need in
everyday life. All subjects improved their FIM scores after the
transplantation-rehabilitation intervention.
D) Anal
Assessment: Of the 15 subjects without anal sensation at the
baseline evaluation, nine recovered some feeling. Before the
intervention, all 20 subjects were unable to contract their anus, an
ability recovered by five afterwards.
E) Bladder
Function: Of the 15 patients without bladder sensation at the
baseline evaluation, five regained the ability to sense bladder
fullness. One patient recovered bladder control.
F) Nerve
Conduction: Electrophysiological evaluations of nerve conduction
indicated that 15 subjects could direct signals to previously paralyzed
muscles.
Side Effects:
Like the earlier study, all subjects eventually recovered smelling
ability. One patient developed meningitis two weeks after surgery and,
as a result, lost sensory and motor function, some of which came
back over time. The investigators suspected that the infection was
caused when the extracted olfactory-tissue sample was withdrawn through
the nasal passages.
Conclusion:
The investigators concluded that olfactory-tissue transplantation is
“feasible, relatively safe, and possibly beneficial in people with
chronic SCI when combined with postoperative rehabilitation.” They also
emphasized that neither rehabilitation nor transplantation alone is
sufficient to promote recovery; both are needed. The results also
suggest that the nature of the post-transplantation rehabilitation is
extraordinarily important.
3) A 2009 article
coauthored by Indian scientists trained by Lima’s team as well as
himself reported the results of an Indian pilot study, which treated
five men with chronic thoracic (4) or cervical injuries (1) over the
November 2006 to January 2008 period. Patient age ranged from 18 to 40
years, and the time lapsing since injury varied from 2.4 to 8.2 years.
Various follow-up assessments similar to those described in the previous
study were carried out before transplantation and afterwards at
half-year intervals up to 18 months, although one patient just had a
six-month assessment at the time the article was submitted.
Unlike the
previous study, functional improvements were generally not observed. The
investigators specifically concluded that although the procedure is
relatively safe and feasible, no “efficacy could be demonstrated which
could be attributed to the procedure.”
In the previous
article, Lima implied that this Indian pilot study may have failed to
generate functional improvements because the study’s
post-transplantation rehabilitation program, which he believes is
extraordinarily important, was ambiguously implemented. Specifically, he
notes that patients were only given instructions to follow a
rehabilitation program at home, and their compliance with it and its
intensity is unknown.
Clearly, when it
comes to this olfactory-tissue approach for restoring function after
SCI, the nature, intensity, and duration of the post-transplantation
rehabilitation program will be one of those extremely important,
“God-is-in-the-details” factors that determines whether success is
forthcoming or not.

2) Dr. Hongyun
Huang (China) has
transplanted olfactory ensheathing cells (OECs) isolated from fetal
olfactory bulbs into more than 1,200 patients from 70+ countries with a
variety of neurological disorders, including 600+ with chronic SCI. The
OECs were isolated from 12-16-week aborted fetuses, and grown and
expanded in culture for 12-17 days. For SCI, about a million cells were
injected around the injury site exposed through a limited laminectomy.
The OECs were often tra nsplanted
many years after injury.
nsplanted
many years after injury.
Because many patients regain some function soon
after surgery, improvement is not due to relatively slow neuronal
regeneration or remyelination. Huang speculates that OECs wakeup
quiescent neurons that still transverse the injury site, perhaps by
altering the injury site’s environment through secreting growth factors
and producing adhesion and matrix molecules.
Huang’s SCI work has been summarized in several
professional articles. In 2003 and 2006 articles, he reported the
results of transplanting OECs into 139 men and 32 women, of which 114
were quadriplegics and 57 paraplegics. Ages ranged from 2 to 64 (average
35) years, and the interval between injury and admission varied from 6
months to18 years. To ensure that improvement was not merely due to
surgery-associated decompression, patient MRIs had to indicate the
absence of compression before surgery. In addition, the cord had to have
some structural continuity through the injury site, the situation for
most individuals with SCI.
Function was assessed before and 2-8 weeks after
surgery using the ASIA (American Spinal Injury Association) impairment
scales, which include motor-function, light-touch, and pin-prick scores.
Improvement was noted for each of these scores in five age categories
(<20, 21-30, 31- 40, 41- 50, and >50).
Another study evaluated the influence of various
factors (e.g., age, sex, time from injury, completeness of injury, and
injury level) on OEC-transplantation effectiveness in 300 patients with
chronic injuries. Once again, most patients demonstrated some motor and
sensory improvement. Those with cervical injuries recovered more
function than those with thoracic injuries. No differences were noted
among the other injury factors examined.
In 2007, Huang reported the results of following 16
OEC recipients (14 men, 2 women) with MRI imaging for an average of 38
months (6). Ten and six had complete and incomplete injuries,
respectively. The time elapsing from injury ranged from 22 to 55 years.
The MRI follow-up imaging of the cord showed the absence of tumors, new
or expanding cysts, infection, or neural disruption at the
transplantation site, findings which supported the procedure’s safety.
In 2012, Huang and his colleagues summarized the
long-term outcomes of treating 108 patients with complete chronic
injuries with OEC transplantation. Eight-four patients were men, and 24
were women; age ranged from 6 to 58 (average 34), and the time injured
before treatment varied from 0.5 to 30 (average 3.5) years. Fifty-one,
42, and 15 had cervical, thoracic, and thoracocolumbar junction (T12-L1)
injuries, respectively. After transplantation, patients were followed
for an average of 3.5 years, using a variety of assessments, including
the the ASIA impairment scales and its component motor-function,
light-touch, and pin-prick scores. Similar to the aforementioned
short-term results, modest improvements were noted on average for each
of these scores. Fourteen of the 108 patients improved from ASIA-A
(complete injury) to ASIA-B (some sensory return), and 18 improved from
ASIA-A to ASIA-C (some sensory and motor function recovery). Nine
patients regained limited ambulatory ability, and 12 of the 84 men had
improved sexual functioning. In general, patients who pursued
aggressived rehabilitation obtained better results.
3) Dr.
Alan Mackay-Sim’s team (Brisbane, Australia), in a single-blind
phase-1 clinical trial, has implanted autologous OECs back into the
patient’s injured cord (Brain, published online October 11, 2005).
 The OECs were isolated from the patient’s nasal tissue and amplified in
culture to yield up to 20-million cells over six weeks.
The OECs were isolated from the patient’s nasal tissue and amplified in
culture to yield up to 20-million cells over six weeks.
 These cells were
injected into 40 sites surrounding the injury site. The progress of three
male subjects (18-55 years of age) with complete thoracic injuries
sustained 6-32 months previously who received OEC transplants were
compared to three individuals who did not have the transplants. These
comparative assessments were blinded, i.e., progress-monitoring assessors
do not know which patients had the procedure. These periodic assessments
included MRI, neurological, psychosocial, ASIA (American Spinal Injury
Association), and FIM (Functional Independence Measure) evaluations. The
investigators concluded “transplantation of autologous olfactory
ensheathing cells into the injured spinal cord is feasible and is safe up
to one year post-implantation.”
These cells were
injected into 40 sites surrounding the injury site. The progress of three
male subjects (18-55 years of age) with complete thoracic injuries
sustained 6-32 months previously who received OEC transplants were
compared to three individuals who did not have the transplants. These
comparative assessments were blinded, i.e., progress-monitoring assessors
do not know which patients had the procedure. These periodic assessments
included MRI, neurological, psychosocial, ASIA (American Spinal Injury
Association), and FIM (Functional Independence Measure) evaluations. The
investigators concluded “transplantation of autologous olfactory
ensheathing cells into the injured spinal cord is feasible and is safe up
to one year post-implantation.”
In 2008, the results of three-years of follow-up
experience were reported. Again, no adverse effects were observed from
the OEC-transplantation procedures. For example, no tumors were observed
nor the development of syringomyelia cysts within the cord (see
glossary). In one patient, improvement was noted in light-touch and
pin-prick sensitivity. The investigators emphasized that it was
important not to over-extrapolate the findings due to the small number
of patients involved in this preliminary trial.
4)Using
the procedures developed by Dr. Huang described above,
Dr. Tiansheng
Sun and colleagues (China) reported the
transplantation of fetal OECs into 11 patients with complete, chronic
SCI (13-14). Nine were men and two were women; age varied from 25 to 55
years; and the interval between injury and transplantation ranged from 2
to 5.5 years. After exposing the cord with a laminectomy, approximately
500,000 cells suspended in 0.5 milliliters were injected at various
locations surrounding the injury site. There were no procedural
complications. Patients were followed for an average of 14 months.
Although locomotor improvement was minimal, sensation improved
moderately as measured by ASIA evaluations, and a number of patients had
less spasticity.
5) Dr.
Wlodzimierz Jarmundowicz, Dr. Pawel Tabakow, and colleagues
(Poland) have initiated a phase-I clinical trial to assess the safety
and feasibility of transplanting autologous OECs (i.e., obtained from
the patient) to treat complete SCI. The procedures were developed on a
foundation of preliminary studies using rats and human cadavers. The
first operation was performed in June 2008 on a 27-year-old male who
sustained a complete (ASIA-A), thoracic T10-11 injury four years earlier
from a knife wound.
OECs were
isolated from the patient’s olfactory tissue and grown and amplified in
culture. Three weeks later, the spinal-cord injury area was exposed
through a two-level laminectomy, fibrous adhesions were removed, and a
cell suspension of OECs and olfactory fibroblasts were microinjected
~120 times into the area surrounding the injury site. Each injection
contained ~25,000 cells. Four weeks after the operation, there were no
adverse effects attributed to the procedures.
 The
patient continues neurorehabilitation.
The
patient continues neurorehabilitation.
A second patient was
similarly treated in August 2008. This individual was a 27-year old male
who sustained a thoracic T6-7, ASIA-A-complete injury five years
earlier. After the cells were cultured for 17 days, they were
reintroduced into the patient’s spinal cord. No adverse complications
were noted in the month following transplantation.
One-year follow-up of these patients indicated that
1) the OEC transplantation was safe and 2) both patients had improved
neurologically. Specifically, the first patient improved from an ASIA-A
(motor and sensory complete injury) to an ASIA-C incomplete injury; and
the second patient improved from ASIA A to ASIA B (i.e., some restored
sensation). In contrast, no control patients have showed improvement.
In June 2010, a third patient, a 26-year-old male
with a complete thoracic T4 injury, was treated in a similar fashion.
A 2013 article
provided more in-depth information on the procedures used in these three
patients, as well as the outcomes observed one year after
transplantation. To ensure that any improvement was not merely the
result of physical rehabilitation, all patients underwent extensive
physical rehabilitation before and after transplantation. Outcomes were
compared to those of three comparably injured subjects, who did not have
the procedure but underwent physical rehabilitation. One year after
transplantation, no adverse effects were observed. Two of the three
transplantation patients improved from ASIA A to ASIA C, and although
the third patient remained at the ASIA-A level, some motor and sensory
improvement accrued. No neurological improvement was observed in
control subjects.
In 2014, the
investigative team reported the transplantation of olfactory cells
obtained not from the patient’s more accessible olfactory mucosal tissue
(i.e., nose) but from an olfactory bulb located under the brain’s
cranium. The 38-year-old male patient had sustained an ASIA-A complete
injury at the thoracic T-9 level 13 months before the procedure due to a
knife assault. The injury had resulted in an eight-millimeter gap in the
spinal cord, the stumps being connected by a thin rim of spared tissue.
An olfactory bulb was obtained through a craniotomy, a surgical
procedure that opens up the skull to access the brain. The bulb was
cultured to obtain a mixture of OECs and olfactory nerve fibroblasts.
After exposing the spinal cord injury-site, scar and tethering tissue
were removed, followed by injection of the cultured cells into multiple
locations surrounding the injury site. Finally, four sural-nerve strips
obtained from the patient’s leg were used to bridge the spinal cord
stumps. The surgery was followed by extended, aggressive physical
rehabilitation. To ensure that any functional improvement was not merely
due to aggressive rehabilitation that had been done after but not before
surgery, the patient underwent similar rehabilitation for eight-months
before the intervention. No neurological improvement accrued during the
pre-surgical period.
In the 19-month
follow-up period, the patient improved from an ASIA-A
motor-and-sensory-complete injury to an ASIA-C incomplete injury. This
upgrading correlated with improved trunk stability, recovery of some
sensation and voluntary lower-extremity movements, and increased muscle
mass. In addition, imaging assessments demonstrated that the nerve
grafts had bridged the gap at the spinal cord injury site. Noting that
it was difficult to determine the contribution of each element of this
multi-pronged intervention to (i.e., untethering and scar removal, cell
transplantation, sural-nerve bridging, and physical rehabilitation), the
investigators believed that all components collectively contributed to
the patient’s neurological improvement.
TOP