1) Craniosacral Therapy
2) Chronological Controlled
Developmental Therapy
3) Massage Therapy
4) Chiropractic Therapy
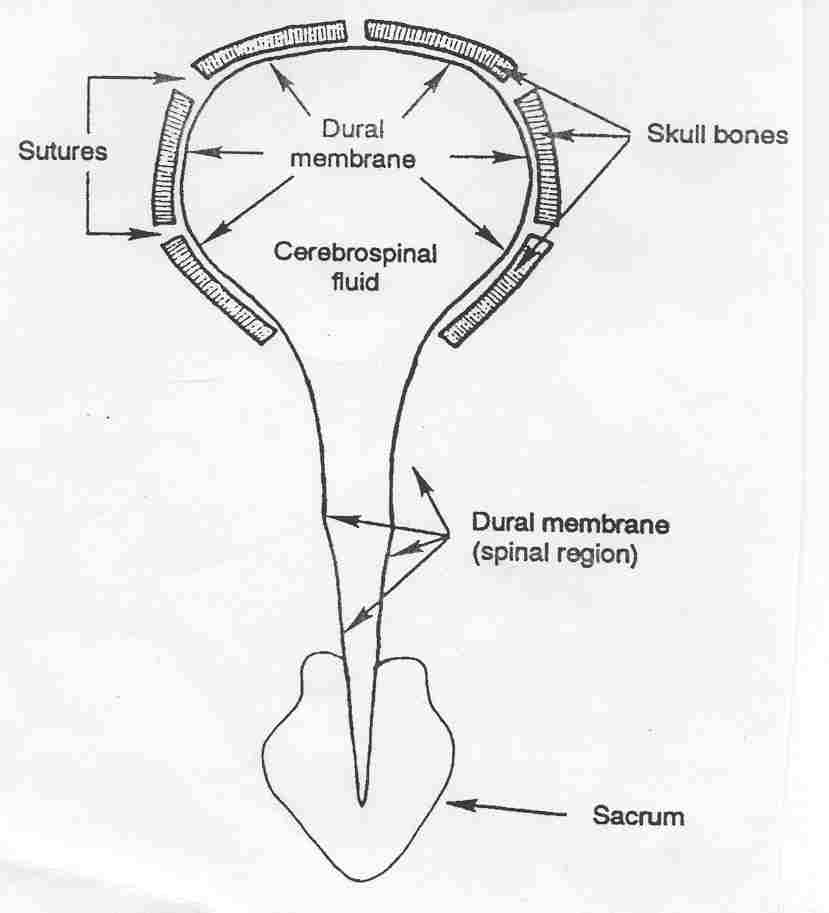
1) Craniosacral
Therapy: Dr. John Upledger (Florida, USA) (photo) developed
craniosacral therapy a gentle hands-on procedure for evaluating and enhancing the functioning of the craniosacral
system. Because the system surrounds the brain and spinal cord, it affects
the entire body and, as such, the therapy has the ability to treat a
wide-range of disorders, including SCI. Therapists use a light touch to
feel the rhythmic motion of the cerebrospinal fluid within the
craniosacral system (click on illustration) and, in turn, to treat any
restrictions. Because a restriction in on
procedure for evaluating and enhancing the functioning of the craniosacral
system. Because the system surrounds the brain and spinal cord, it affects
the entire body and, as such, the therapy has the ability to treat a
wide-range of disorders, including SCI. Therapists use a light touch to
feel the rhythmic motion of the cerebrospinal fluid within the
craniosacral system (click on illustration) and, in turn, to treat any
restrictions. Because a restriction in on e
area can affect the entire system, treatment may involve working at a
point distant from the overt symptoms.
e
area can affect the entire system, treatment may involve working at a
point distant from the overt symptoms.
Many treated patients with SCI report improvements,
ranging from modest to fairly dramatic, involving motor function, bowel
and bladder control, spasticity management, and overall well-being and
ease.

2) Chronological Controlled
Developmental Therapy (CCDT): Ed Snapp, (Mississippi, USA) a physical
 therapist
who acquired polio in his youth, developed CCDT, a bodywork therapy that
targets various neurological disorders, including SCI (photo of Snapp by
hydrotherapy tank). It consists of a number of fairly standard physical
therapies performed in a defined sequence, including pressure stimulation,
hydrotherapy, light-touch massage, movements on an oil table, and rest in
a sling apparatus that mimics a fetal position. The therapies are done to
the patient, who exerts no effort, and carried out in a distraction-free
environment.
therapist
who acquired polio in his youth, developed CCDT, a bodywork therapy that
targets various neurological disorders, including SCI (photo of Snapp by
hydrotherapy tank). It consists of a number of fairly standard physical
therapies performed in a defined sequence, including pressure stimulation,
hydrotherapy, light-touch massage, movements on an oil table, and rest in
a sling apparatus that mimics a fetal position. The therapies are done to
the patient, who exerts no effort, and carried out in a distraction-free
environment.
Under CCDT theory, turning on dormant neurons
requires a sequence of cues that mimic events from our early fetal and
infant development, which, in turn, reflect a genetic memory of our
evolutionary development. If a fully developed neuron has been turned
off, its reactivation requires that it receive and sense external cues in
a defined sequence that are correlated to the neuron’s initial
development. There is no avenue to deliver these cues except through the
peripheral senses. Out-of-sequence cues will not work.
3) Massage Therapy: Dr.
Tiffany Field and colleagues (Florida, USA) have shown that subjects with
cervical level (C5-7) injuries benefited from a five-week program of twice
weekly, 40-minute massage sessions (Diego MA et al, Intern J
Neuroscience 112, 2002). After stratification by range of motion, 20
subjects were randomly assigned to either a massage therapy or exercise
group. Fifteen were males; average age was 39, and all had been injured
for at least a year – i.e., chronic injuries. Results indicated that the
massage-therapy group compared to the exercise group had less depression
and anxiety and increased muscle strength and range of motion.
4) Chiropractic
Therapy: According to a Kessler Institute (New Jersey, USA) study, 23%
of people with SCI with chronic pain had used chiropractic (Nayak et al,
J. Spinal Cord Medicine, Spring, 2001). Chiropractic therapy
usually focuses on areas above the injury site, although more passive
mobilization may be applied to areas below the injury such as the pelvis,
low back, and lower extremities. The overall goal is to enhance the range
of motion often compromised by excessive shoulder and arm use often
associated with frequent wheelchair transfers and which can lead to more
serious repetitive-use injuries. Chiropractic adjustments, muscle work,
and exercises keep the spine, shoulders, ribs, and shoulder blades moving
as they should in a painless, full range of motion. These methods keep
the joints lubricated, discs between the vertebrae from deteriorating, and
muscles and ligaments strong and balanced.
TOP